

Pediatric Procedural Sedation Using the Combination of Ketamine and Propofol Outside of the Emergency Department: A Report From the Pediatric Sedation Research Consortium
- PMID: 28650904
- PMCID: PMC6287759
- DOI: 10.1097/PCC.0000000000001246
Pediatric Procedural Sedation Using the Combination of Ketamine and Propofol Outside of the Emergency Department: A Report From the Pediatric Sedation Research Consortium
Abstract
Objectives: Outcomes associated with a sedative regimen comprised ketamine + propofol for pediatric procedural sedation outside of both the pediatric emergency department and operating room are underreported. We used the Pediatric Sedation Research Consortium database to describe a multicenter experience with ketamine + propofol by pediatric sedation providers.
Design: Prospective observational study of children receiving IV ketamine + propofol for procedural sedation outside of the operating room and emergency department using data abstracted from the Pediatric Sedation Research Consortium during 2007-2015.
Setting: Procedural sedation services from academic, community, free-standing children's hospitals, and pediatric wards within general hospitals.
Patients: Children from birth to less than or equal to 21 years old.
Interventions: None.
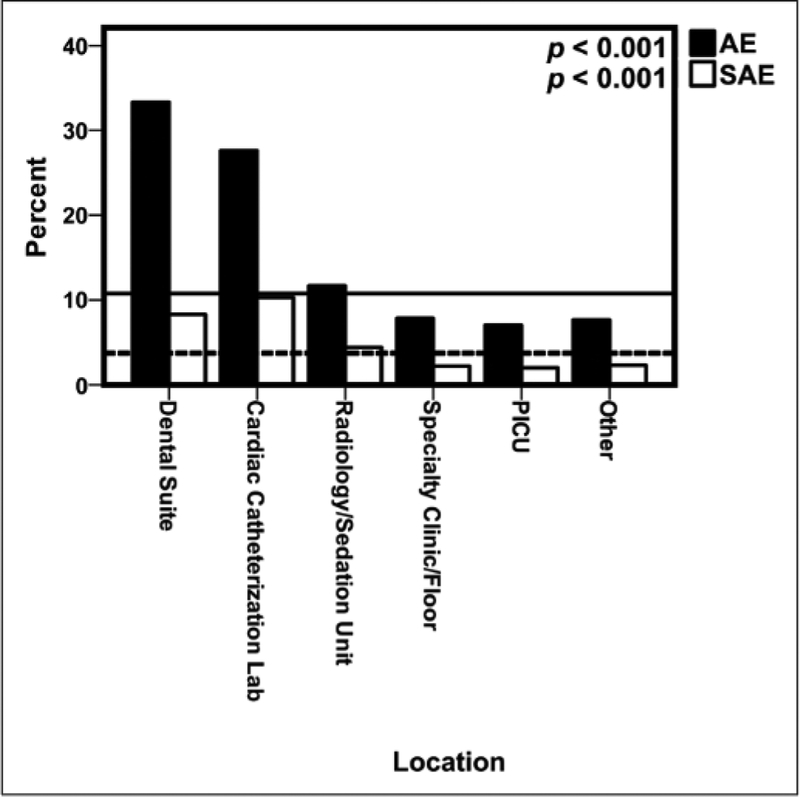
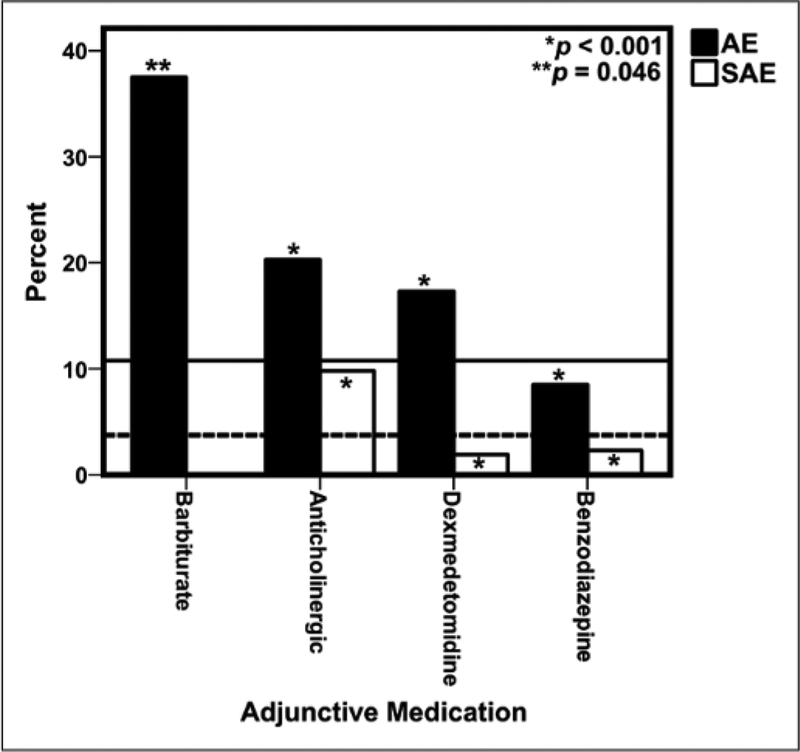
Measurements and main results: A total of 7,313 pediatric procedural sedations were performed using IV ketamine + propofol as the primary sedative regimen. Median age was 84 months (range, < 1 mo to ≤ 21 yr; interquartile range, 36-144); 80.6% were American Society of Anesthesiologists-Physical Status less than III. The majority of sedation was performed in dedicated sedation or radiology units (76.1%). Procedures were successfully completed in 99.8% of patients. Anticholinergics (glycopyrrolate and atropine) or benzodiazepines (midazolam and lorazepam) were used in 14.2% and 41.3%, respectively. The overall adverse event and serious adverse event rates were 9.79% (95% CI, 9.12-10.49%) and 3.47% (95% CI, 3.07-3.92%), respectively. No deaths occurred. Risk factors associated with an increase in odds of adverse event included ASA status greater than or equal to III, dental suite, cardiac catheterization laboratory or radiology/sedation suite location, a primary diagnosis of having a gastrointestinal illness, and the coadministration of an anticholinergic.
Conclusions: Using Pediatric Sedation Research Consortium data, we describe the diverse use of IV ketamine + propofol for procedural sedation in the largest reported cohort of children to date. Data from this study may be used to design sufficiently powered prospective randomized, double-blind studies comparing outcomes of sedation between commonly administered sedative and analgesic medication regimens.
Figures
References
-
- Coté CJ: American Academy of Pediatrics sedation guidelines: Are we there yet? Arch Pediatr Adolesc Med 2012; 166:1067–1069 - PubMed
-
- Cravero JP: Pediatric sedation with propofol-continuing evolution of procedural sedation practice. J Pediatr 2012; 160:714–716 - PubMed
-
- Cravero JP, Beach ML, Blike GT, et al. ; Pediatric Sedation Research Consortium: The incidence and nature of adverse events during pediatric sedation/anesthesia with propofol for procedures outside the operating room: A report from the Pediatric Sedation Research Consortium. Anesth Analg 2009; 108:795–804 - PubMed
-
- Green SM, Roback MG, Krauss B, et al. ; Emergency Department Ketamine Meta-Analysis Study Group: Predictors of emesis and recovery agitation with emergency department ketamine sedation: An individual-patient data meta-analysis of 8,282 children. Ann Emerg Med 2009; 54:171–80.e1 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
