

Randomized Trial of Reducing Ambulatory Malpractice and Safety Risk: Results of the Massachusetts PROMISES Project
- PMID: 28650922
- PMCID: PMC5739317
- DOI: 10.1097/MLR.0000000000000759
Randomized Trial of Reducing Ambulatory Malpractice and Safety Risk: Results of the Massachusetts PROMISES Project
Abstract
Objective: Evaluate application of quality improvement approaches to key ambulatory malpractice risk and safety areas.
Study setting: In total, 25 small-to-medium-sized primary care practices (16 intervention; 9 control) in Massachusetts.
Study design: Controlled trial of a 15-month intervention including exposure to a learning network, webinars, face-to-face meetings, and coaching by improvement advisors targeting "3+1" high-risk domains: test result, referral, and medication management plus culture/communication issues evaluated by survey and chart review tools.
Data collection methods: Chart reviews conducted at baseline and postintervention for intervention sites. Staff and patient survey data collected at baseline and postintervention for intervention and control sites.
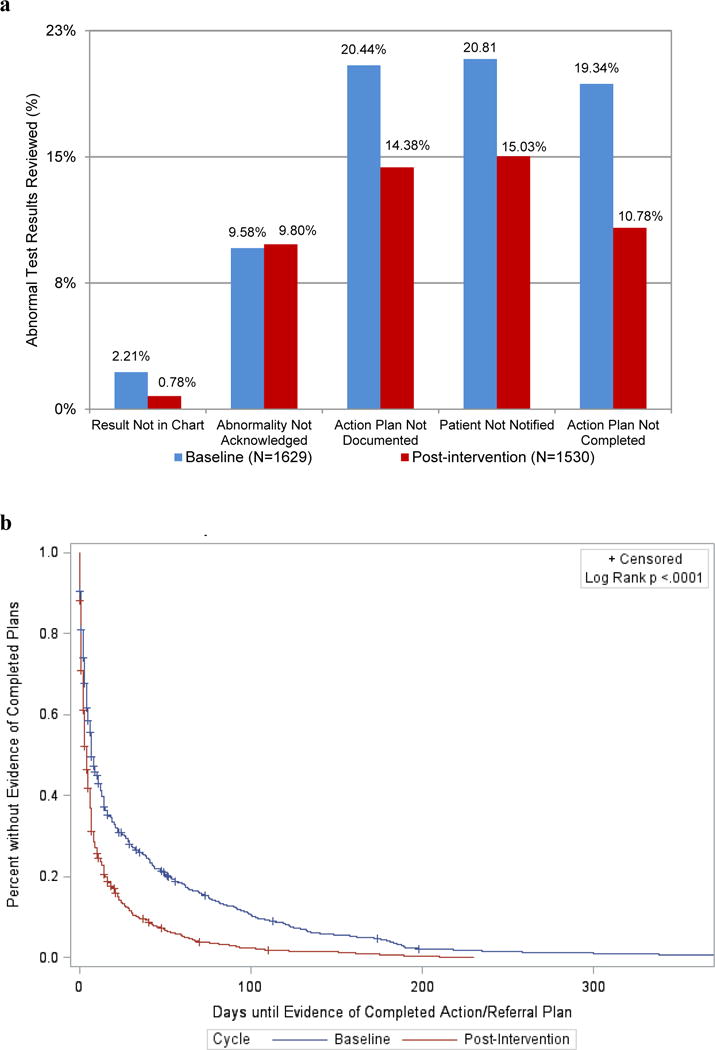
Principal findings: Chart reviews demonstrated significant improvements in documentation of abnormal results, patient notification, documentation of an action or treatment plan, and evidence of a completed plan (all P<0.001). Mean days between laboratory test date and evidence of completed action/treatment plan decreased by 19.4 days (P<0.001). Staff surveys showed modest but nonsignificant improvement for intervention practices relative to controls overall and for the 3 high-risk domains that were the focus of PROMISES.
Conclusions: A consortium of stakeholders, quality improvement tools, coaches, and learning network decreased selected ambulatory safety risks often seen in malpractice claims.
Conflict of interest statement
Figures
References
-
- Gandhi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med. 2006;5:488–96. - PubMed
-
- Gandhi TK, Lee TH. Patient safety beyond the hospital. N Engl J Med. 2010;363:1001–3. - PubMed
-
- Wynia MK, Classen DC. Improving ambulatory patient safety: learning from the last decade, moving ahead in the next. JAMA. 2011;306:2504–5. - PubMed
-
- Zuccotti G, Sato L. Malpractice risk in ambulatory settings: an increasing and underrecognized problem. JAMA. 2011;305:2464–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
