

Point-of-care testing for Toxoplasma gondii IgG/IgM using Toxoplasma ICT IgG-IgM test with sera from the United States and implications for developing countries
- PMID: 28650970
- PMCID: PMC5501679
- DOI: 10.1371/journal.pntd.0005670
Point-of-care testing for Toxoplasma gondii IgG/IgM using Toxoplasma ICT IgG-IgM test with sera from the United States and implications for developing countries
Abstract
Background: Congenital toxoplasmosis is a serious but preventable and treatable disease. Gestational screening facilitates early detection and treatment of primary acquisition. Thus, fetal infection can be promptly diagnosed and treated and outcomes can be improved.
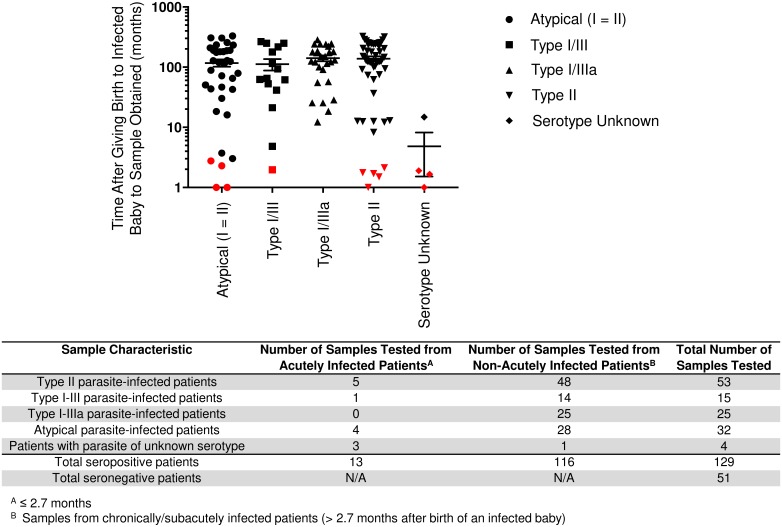
Methods: We tested 180 sera with the Toxoplasma ICT IgG-IgM point-of-care (POC) test. Sera were from 116 chronically infected persons (48 serotype II; 14 serotype I-III; 25 serotype I-IIIa; 28 serotype Atypical, haplogroup 12; 1 not typed). These represent strains of parasites infecting mothers of congenitally infected children in the U.S. 51 seronegative samples and 13 samples from recently infected persons known to be IgG/IgM positive within the prior 2.7 months also were tested. Interpretation was confirmed by two blinded observers. A comparison of costs for POC vs. commercial laboratory testing methods was performed.
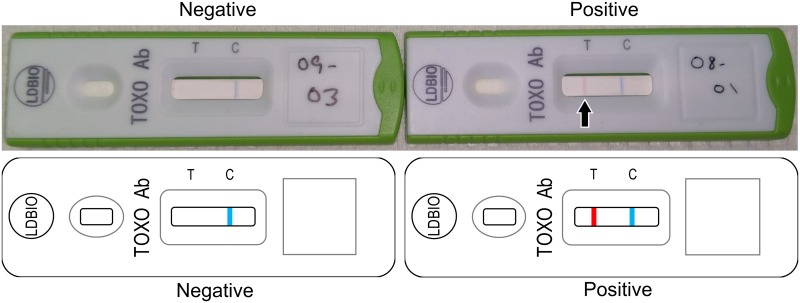
Results: We found that this new Toxoplasma ICT IgG-IgM POC test was highly sensitive (100%) and specific (100%) for distinguishing IgG/IgM-positive from negative sera. Use of such reliable POC tests can be cost-saving and benefit patients.
Conclusions: Our work demonstrates that the Toxoplasma ICT IgG-IgM test can function reliably as a point-of-care test to diagnose Toxoplasma gondii infection in the U.S. This provides an opportunity to improve maternal-fetal care by using approaches, diagnostic tools, and medicines already available. This infection has serious, lifelong consequences for infected persons and their families. From the present study, it appears a simple, low-cost POC test is now available to help prevent morbidity/disability, decrease cost, and make gestational screening feasible. It also offers new options for improved prenatal care in low- and middle-income countries.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: Dr. Rima McLeod is working on a literature review for Sanofi Pasteur.
Figures

References
-
- Lykins J, Wang K, Wheeler K, Clouser F, Dixon A, El Bissati K, et al. Understanding Toxoplasmosis in the United States Through "Large Data" Analyses. Clin Infect Dis. 2016;63(4):468–75. doi: 10.1093/cid/ciw356 - DOI - PMC - PubMed
-
- McLeod R, Lee D, Clouser F, Boyer K. Toxoplasmosis in the Fetus and Newborn Infant In: Stevenson DK, Cohen RS, Sunshine P, editors. Neonatology: Clinical Practice and Procedures. 1st ed New York: McGraw Hill; 2015. p. 821–76.
-
- Montoya JG, Remington JS. Management of Toxoplasma gondii infection during pregnancy. Clin Infect Dis. 2008;47(4):554–66. doi: 10.1086/590149 - DOI - PubMed
-
- Torgerson PR, Mastroiacovo P. The global burden of congenital toxoplasmosis: a systematic review. Bull World Health Organ. 2013;91(7):501–8. doi: 10.2471/BLT.12.111732 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
