

Nonvitamin K antagonist oral anticoagulant use in patients with renal impairment
- PMID: 28651452
- PMCID: PMC5562140
- DOI: 10.1177/1753944717714921
Nonvitamin K antagonist oral anticoagulant use in patients with renal impairment
Abstract
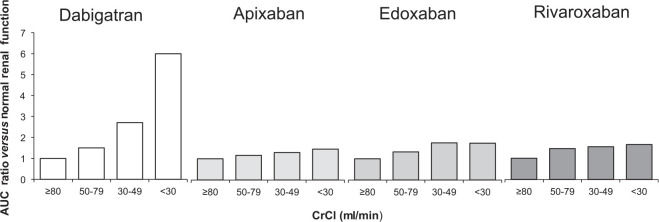
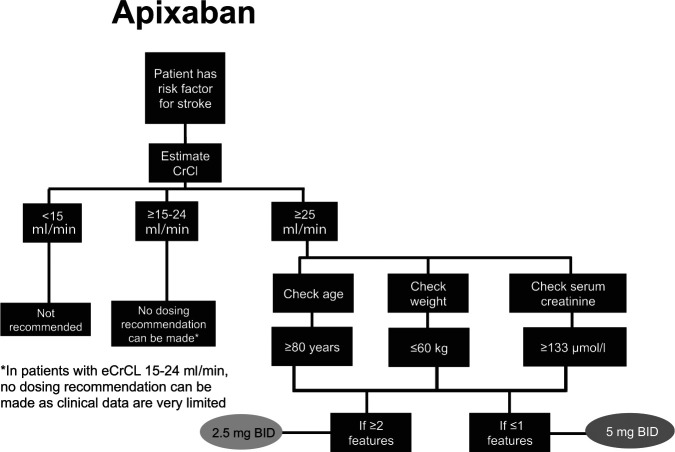
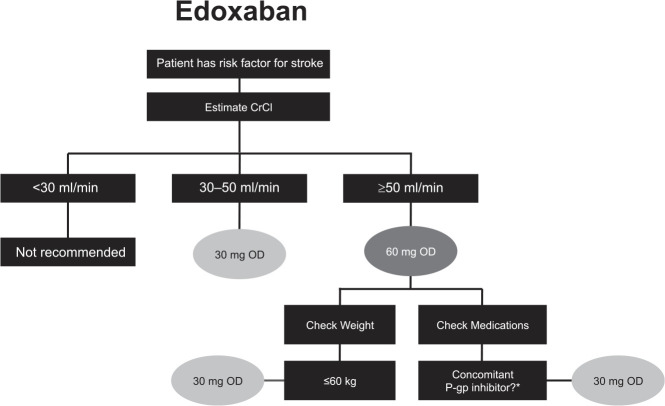
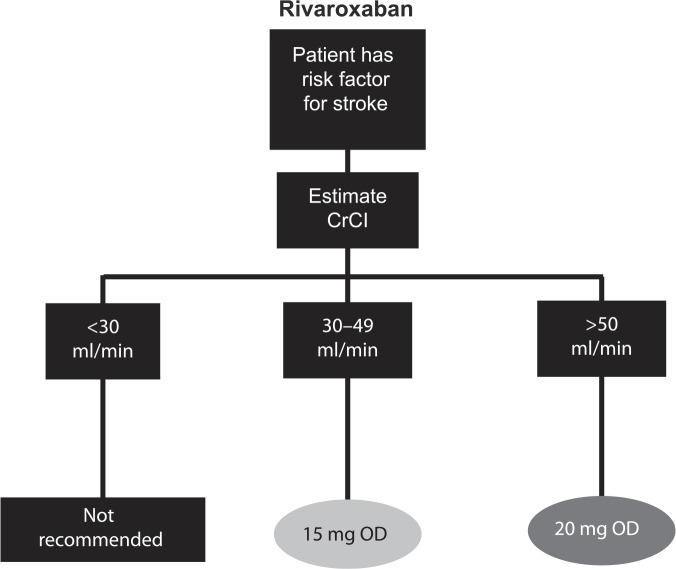
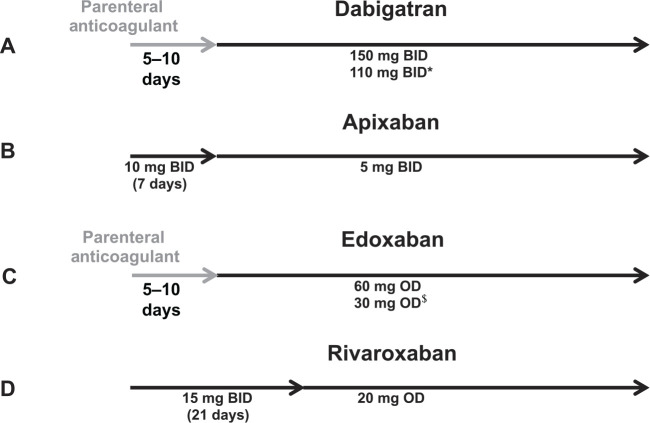
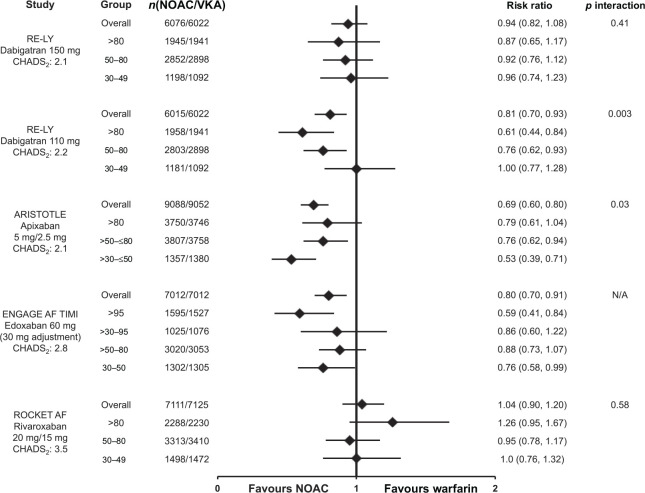
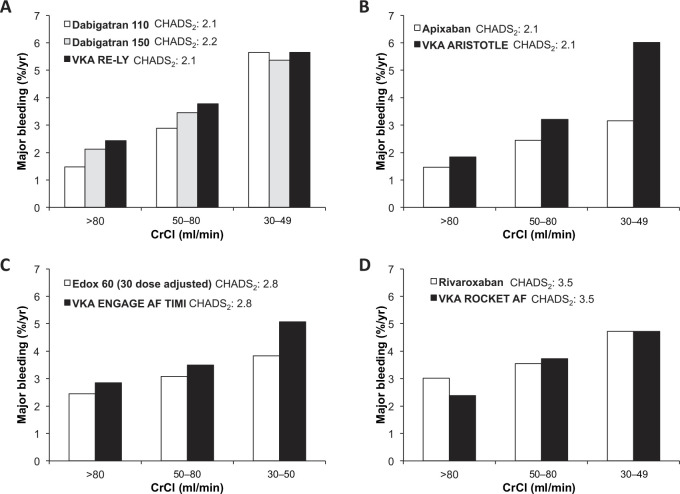
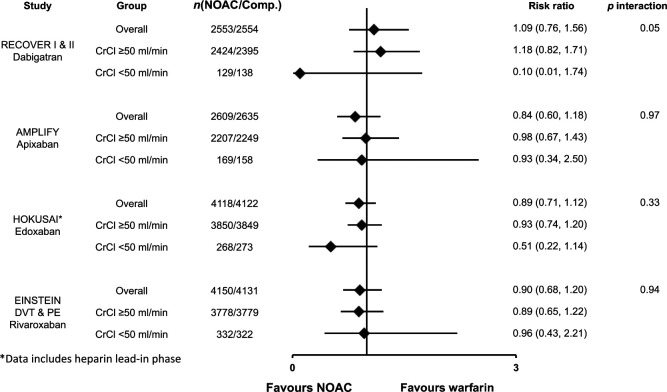
The nonvitamin K antagonist oral anticoagulants (NOACs), also referred to as direct oral anticoagulants (DOACs), dabigatran, apixaban, edoxaban, and rivaroxaban, have emerged as effective alternatives to vitamin K antagonists (VKAs) across several indications, including the prevention of stroke and systemic embolism (SSE) in patients with atrial fibrillation (AF) and the treatment of venous thromboembolism (VTE). Their use in patients with renal impairment is of particular importance, given the prevalence of renal dysfunction in the indicated populations and the impact of renal function on the metabolism of the NOACs. This publication reviews the pharmacokinetic/pharmacodynamic properties of the NOACs and clinical trial results for patients with renal impairment within the AF and VTE indications. Pharmacokinetic/pharmacodynamic data show the NOACs are dependent on renal clearance to varying extents. Relative to VKAs, the efficacy and safety of the NOACs is preserved in patients with moderate renal impairment. The dosing recommendations for patients with renal impairment differ depending on the NOAC, whereby some of the NOACs require dose reductions based solely on renal function, while others require consideration of additional criteria. However, despite these specific dosing recommendations, emerging real-world evidence suggests patients are not being dosed appropriately, indicating a possible knowledge gap. Adherence to recommended dosing algorithms has implications on the optimal efficacy and safety of the NOACs. To this end, renal function should be assessed in patients on a NOAC, as worsening of renal function may warrant change in the dose of a NOAC or change in oral anticoagulant.
Keywords: NOAC; anticoagulation; nonvalvular atrial fibrillation; nonvitamin K antagonist oral anticoagulant; renal impairment; venous thromboembolism.
Conflict of interest statement
Figures



References
-
- Verma A, Cairns JA, Mitchell LB, et al. 2014 focused update of the Canadian Cardiovascular Society Guidelines for the management of atrial fibrillation. Can J Cardiol 2014; 30: 1114–1130. - PubMed
-
- Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013; 369: 2093–2104. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365: 883–891. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009; 361: 1139–1151. - PubMed
-
- Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011; 365: 981–992. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
