

Doxorubicin plus evofosfamide versus doxorubicin alone in locally advanced, unresectable or metastatic soft-tissue sarcoma (TH CR-406/SARC021): an international, multicentre, open-label, randomised phase 3 trial
- PMID: 28651927
- PMCID: PMC7771354
- DOI: 10.1016/S1470-2045(17)30381-9
Doxorubicin plus evofosfamide versus doxorubicin alone in locally advanced, unresectable or metastatic soft-tissue sarcoma (TH CR-406/SARC021): an international, multicentre, open-label, randomised phase 3 trial
Erratum in
-
Correction to Lancet Oncol 2017; 18: 1089-103.Lancet Oncol. 2018 Feb;19(2):e78. doi: 10.1016/S1470-2045(18)30037-8. Lancet Oncol. 2018. PMID: 29413479 No abstract available.
Abstract
Background: Evofosfamide is a hypoxia-activated prodrug of bromo-isophosphoramide mustard. We aimed to assess the benefit of adding evofosfamide to doxorubicin as first-line therapy for advanced soft-tissue sarcomas.
Methods: We did this international, open-label, randomised, phase 3, multicentre trial (TH CR-406/SARC021) at 81 academic or community investigational sites in 13 countries. Eligible patients were aged 15 years or older with a diagnosis of an advanced unresectable or metastatic soft-tissue sarcoma, of intermediate or high grade, for which no standard curative therapy was available, an Eastern Cooperative Oncology Group performance status of 0-1, and measurable disease by Response Evaluation Criteria in Solid Tumors version 1.1. Patients were randomly assigned (1:1) to receive doxorubicin alone (75 mg/m2 via bolus injection administered over 5-20 min or continuous intravenous infusion for 6-96 h on day 1 of every 21-day cycle for up to six cycles) or doxorubicin (given via the same dose procedure) plus evofosfamide (300 mg/m2 intravenously for 30-60 min on days 1 and 8 of every 21-day cycle for up to six cycles). After six cycles of treatment, patients in the single-drug doxorubicin group were followed up expectantly whereas patients with stable or responsive disease in the combination group were allowed to continue with evofosfamide monotherapy until documented disease progression. A web-based central randomisation with block sizes of two and four was stratified by extent of disease, doxorubicin administration method, and previous systemic therapy. Patients and investigators were not masked to treatment assignment. The primary endpoint was overall survival, analysed in the intention-to-treat population. Safety analyses were done in all patients who received any amount of study drug. This study was registered with ClinicalTrials.gov, number NCT01440088.
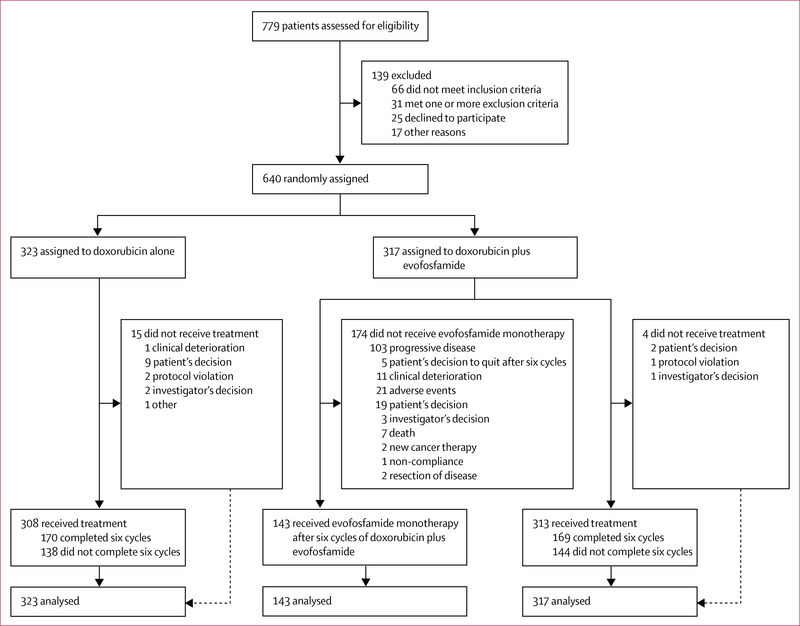
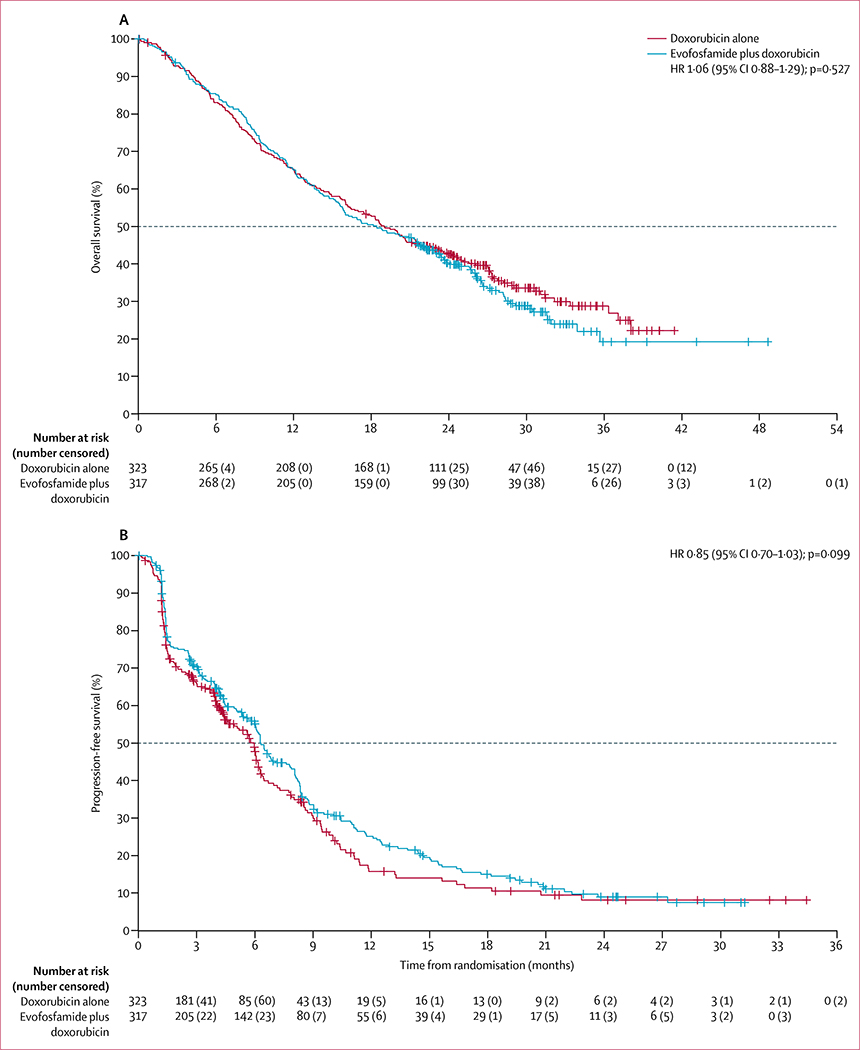
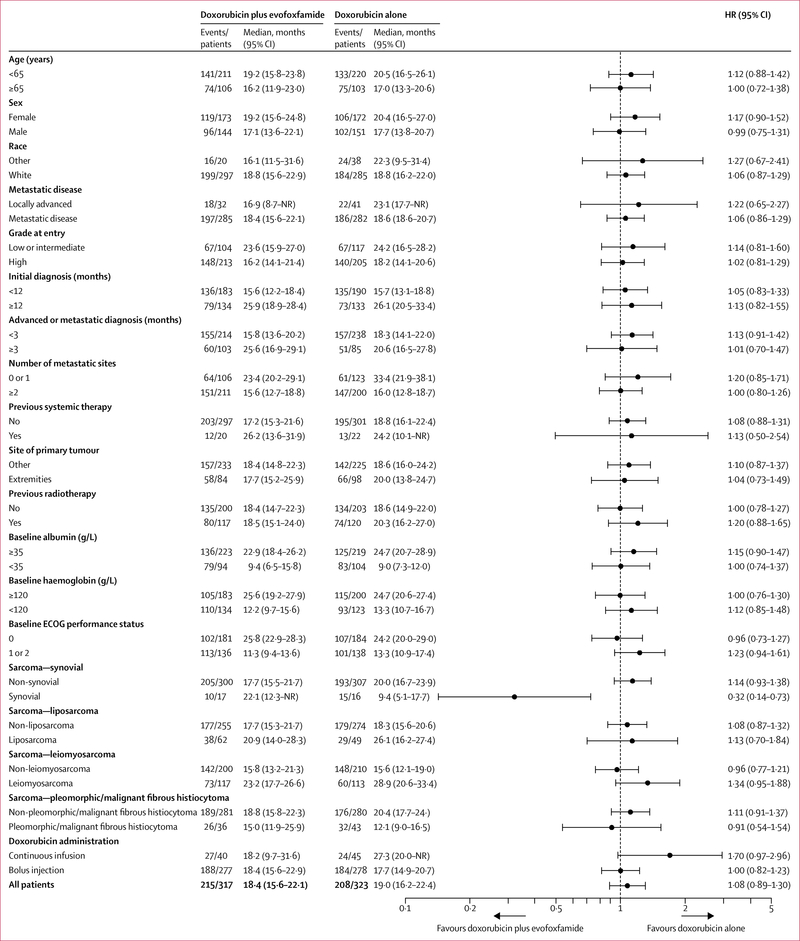
Findings: Between Sept 26, 2011, and Jan 22, 2014, 640 patients were enrolled and randomly assigned to a treatment group (317 to doxorubicin plus evofosfamide and 323 to doxorubicin alone), all of whom were included in the intention-to-treat analysis. The overall survival endpoint was not reached (hazard ratio 1·06, 95% CI 0·88-1·29; p=0·527), with a median overall survival of 18·4 months (95% CI 15·6-22·1) with doxorubicin plus evofosfamide versus 19·0 months (16·2-22·4) with doxorubicin alone. The most common grade 3 or worse adverse events in both groups were haematological, including anaemia (150 [48%] of 313 patients in the doxorubicin plus evofosfamide group vs 65 [21%] of 308 in the doxorubicin group), neutropenia (47 [15%] vs 92 [30%]), febrile neutropenia (57 [18%] vs 34 [11%]), leucopenia (22 [7%] vs 17 [6%]), decreased neutrophil count (31 [10%] vs 41 [13%]), and decreased white blood cell count (39 [13%] vs 33 [11%]). Grade 3-4 thrombocytopenia was more common in the combination group (45 [14%]) than in the doxorubicin alone group (four [1%]), as was grade 3-4 stomatitis (26 [8%] vs seven [2%]). Serious adverse events were reported in 145 (46%) of 313 patients in the combination group and 99 (32%) of 308 in the doxorubicin alone group. Five (2%) patients died from treatment-related causes in the combination group (sepsis [n=2], septic shock [n=1], congestive cardiac failure [n=1], and unknown cause [n=1]) versus one (<1%) patient in the doxorubicin alone group (lactic acidosis [n=1]).
Interpretation: The addition of evofosfamide to doxorubicin as first-line therapy did not improve overall survival compared with single-drug doxorubicin in patients with locally advanced, unresectable, or metastatic soft-tissue sarcomas and so this combination cannot be recommended in this setting.
Funding: Threshold Pharmaceuticals.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Hypoxia-activated prodrug: an appealing preclinical concept yet lost in clinical translation.Lancet Oncol. 2017 Aug;18(8):991-993. doi: 10.1016/S1470-2045(17)30401-1. Epub 2017 Jun 23. Lancet Oncol. 2017. PMID: 28651928 No abstract available.
References
-
- Judson I, Verweij J, Gelderblom H, et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: a randomised controlled phase 3 trial. Lancet Oncol 2014; 15: 415–23. - PubMed
-
- Ryan CW, Merimsky O, Agulnik M, et al. PICASSO III: a phase III, placebo-controlled study of doxorubicin with or without palifosfamide in patients with metastatic soft tissue sarcoma. J Clin Oncol 2016; 34: 3898–905. - PubMed
-
- Seddon BM, Whalen J, Strauss SJ, et al. GeDDiS: a prospective randomised controlled phase III trial of gemcitabine and docetaxel compared with doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft tissue sarcomas. Proc Am Soc Clin Oncol 2015; 33 (suppl): abstr 10500. - PMC - PubMed
-
- Benjamin RS, Wiernik PH, Bachur NR. Adriamycin chemotherapy—efficacy, safety, and pharmacologic basis of an intermittent single high-dosage schedule. Cancer 1974; 33: 19–27. - PubMed
-
- Lorigan P, Verweij J, Papai Z, et al. Phase III trial of two investigational schedules of ifosfamide compared with standard-dose doxorubicin in advanced or metastatic soft tissue sarcoma: a European Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group Study. J Clin Oncol 2007; 25: 3144–50. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
