

Patellofemoral pain in athletes
- PMID: 28652829
- PMCID: PMC5476763
- DOI: 10.2147/OAJSM.S133406
Patellofemoral pain in athletes
Abstract
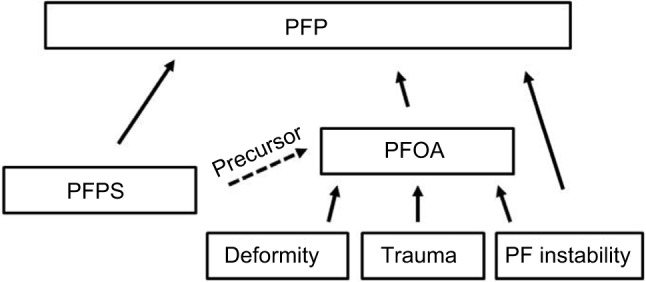
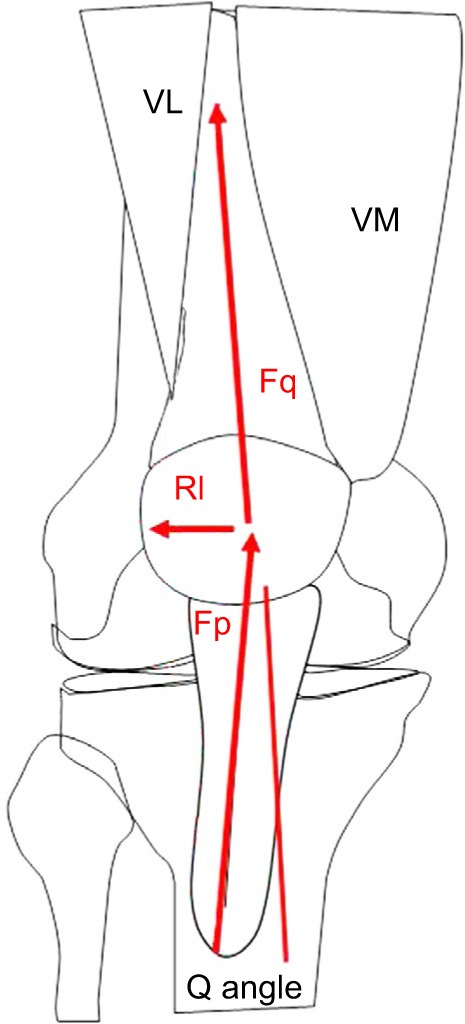
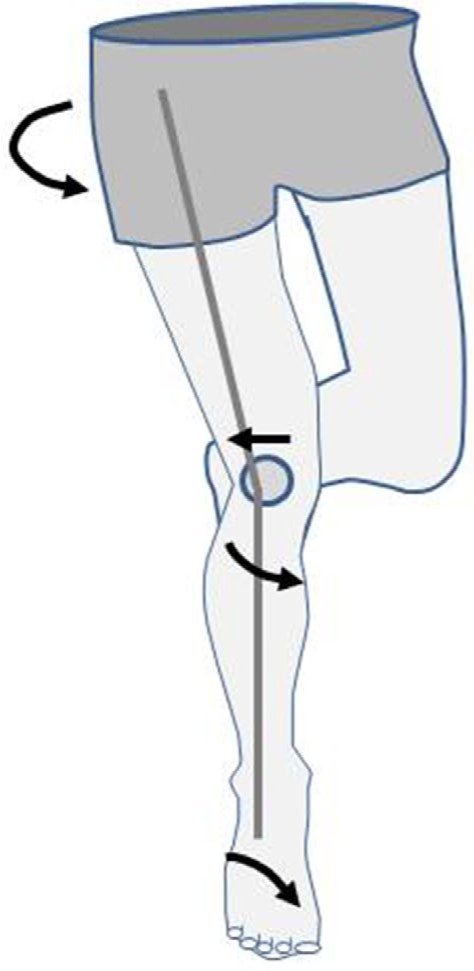
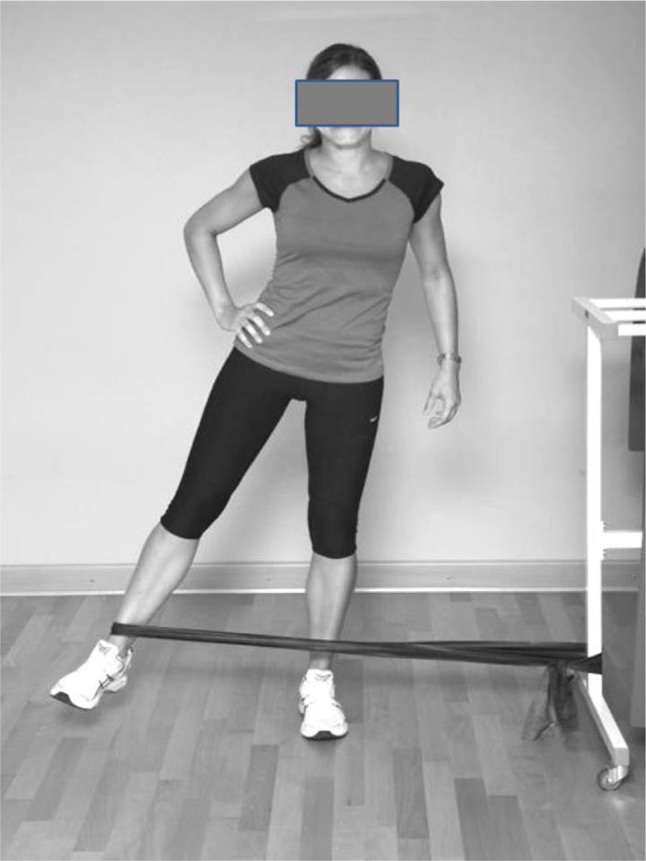
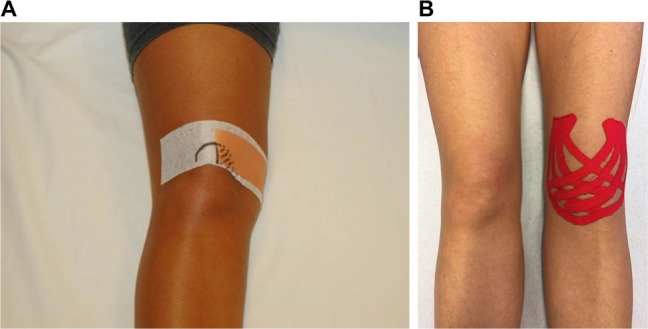
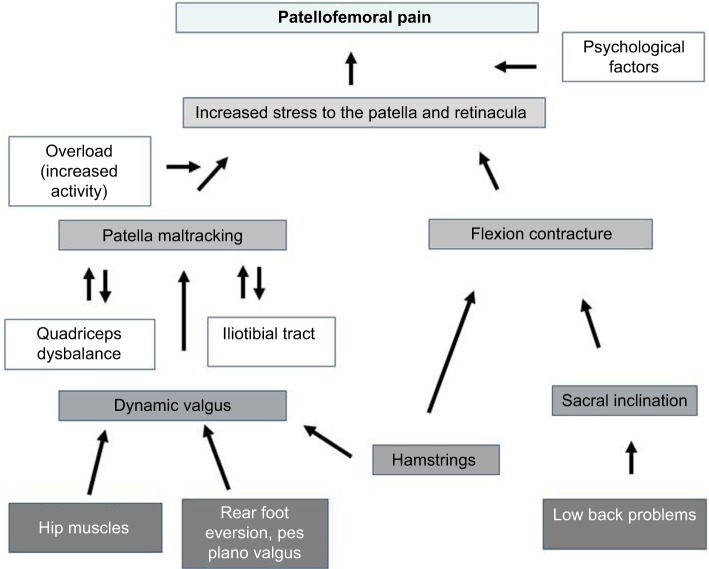
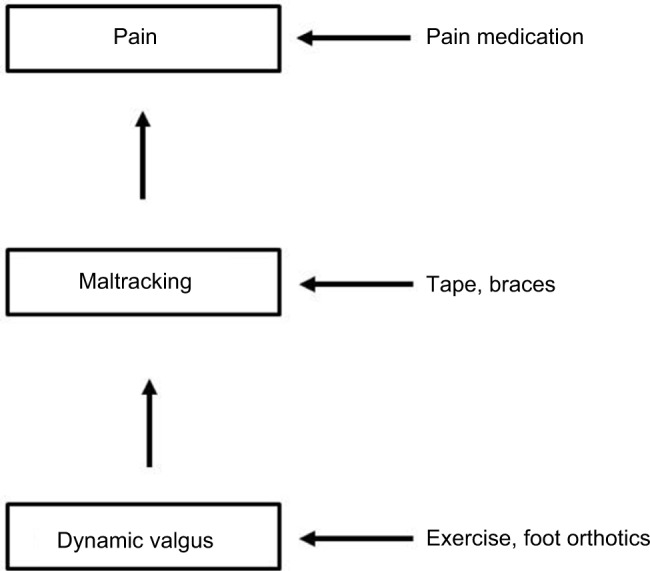
Patellofemoral pain (PFP) is a frequent cause of anterior knee pain in athletes, which affects patients with and without structural patellofemoral joint (PFJ) damage. Most younger patients do not have any structural changes to the PFJ, such as an increased Q angle and a cartilage damage. This clinical entity is known as patellofemoral pain syndrome (PFPS). Older patients usually present with signs of patellofemoral osteoarthritis (PFOA). A key factor in PFPS development is dynamic valgus of the lower extremity, which leads to lateral patellar maltracking. Causes of dynamic valgus include weak hip muscles and rearfoot eversion with pes pronatus valgus. These factors can also be observed in patients with PFOA. The available evidence suggests that patients with PFP are best managed with a tailored, multimodal, nonoperative treatment program that includes short-term pain relief with nonsteroidal anti-inflammatory drugs (NSAIDs), passive correction of patellar maltracking with medially directed tape or braces, correction of the dynamic valgus with exercise programs that target the muscles of the lower extremity, hip, and trunk, and the use of foot orthoses in patients with additional foot abnormalities.
Keywords: anterior knee pain; dynamic valgus; hip strength; rearfoot eversion; single leg squat.
Conflict of interest statement
Disclosure Wolf Petersen, Ingo Rembitzki, and Christian Liebau receive consultant fees from Otto Bock Health Care (Duderstadt, Germany). The authors report no other conflicts of interest in this work.
Figures


References
-
- Crossley KM, Stefanik JJ, Selfe J, et al. Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br J Sports Med. 2016;50(14):839–843. - PMC - PubMed
-
- Crossley KM, van Middelkoop M, Callaghan MJ, et al. Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 2: recommended physical interventions (exercise, taping, bracing, foot orthoses and combined interventions) Br J Sports Med. 2016;50(14):844–852. - PMC - PubMed
-
- Clement DB, Tauton JE, Smart GW, McNicol KL. A survey of overuse running injuries. Phys Sportsmed. 1981;9(1):47–58. - PubMed
-
- Dierks TA, Manal KT, Hamill J, Davis I. Lower extremity kinematics in runners with patellofemoral pain during a prolonged run. Med Sci Sports Exerc. 2011;43(4):693–700. - PubMed
-
- Rathleff MS, Rasmussen S, Olesen JL. Unsatisfactory long-term prognosis of conservative treatment of patellofemoral pain syndrome. Ugeskr Laeger. 2012;174(15):1008–1013. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
