

Abdominal cross-sectional imaging of the associating liver partition and portal vein ligation for staged hepatectomy procedure
- PMID: 28652892
- PMCID: PMC5468342
- DOI: 10.4254/wjh.v9.i16.733
Abdominal cross-sectional imaging of the associating liver partition and portal vein ligation for staged hepatectomy procedure
Abstract
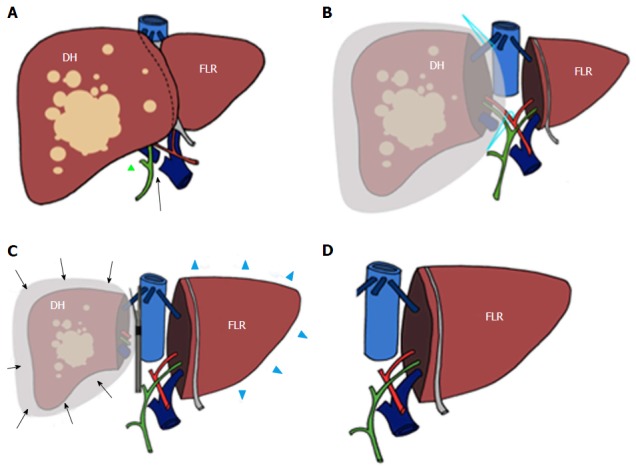
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) is a recently introduced technique aimed to perform two-stage hepatectomy in patients with a variety of primary or secondary neoplastic lesions. ALPSS is based on a preliminary liver resection associated with ligation of the portal branch directed to the diseased hemiliver (DH), followed by hepatectomy after an interval of time in which the future liver remnant (FLR) hypertrophied adequately (partly because of preserved arterialization of the DH). Multidetector computed tomography (MDCT) and magnetic resonance imaging (MRI) play a pivotal role in patients' selection and FLR assessment before and after the procedure, as well as in monitoring early and late complications, as we aim to review in this paper. Moreover, we illustrate main abdominal MDCT and MRI findings related to ALPPS.
Keywords: Associating liver partition and portal vein ligation for staged hepatectomy; Computed tomography; Hepatectomy; Liver surgery; Magnetic resonance imaging.
Conflict of interest statement
Conflict-of-interest statement: None of the authors has conflicts of interest to disclose. This paper has been presented as an electronic poster at the European Congress of Radiology (ECR) 2016 and European Society of Gastrointestinal and Abdominal Radiology (ESGAR) annual meeting 2016.
Figures








References
-
- Agrawal S, Belghiti J. Oncologic resection for malignant tumors of the liver. Ann Surg. 2011;253:656–665. - PubMed
-
- Schnitzbauer A, Lang S A, Fichtner-Feigl S, Loss M, Kroemer A, Goessmann H, Farkas SA, Kirchner G, Jung EM, Scherer MN, et al. Berlin: Oral Presentation; 2010. In situ split with portal vein ligation induces rapid left lateral lobe hypertrophy enabling two-staged extended right hepatic resection; p. 35.
-
- Herman P, Krüger JA, Perini MV, Coelho FF, Cecconello I. High Mortality Rates After ALPPS: the Devil Is the Indication. J Gastrointest Cancer. 2015;46:190–194. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
