

Neuroclinical Framework for the Role of Stress in Addiction
- PMID: 28653044
- PMCID: PMC5482275
- DOI: 10.1177/2470547017698140
Neuroclinical Framework for the Role of Stress in Addiction
Abstract
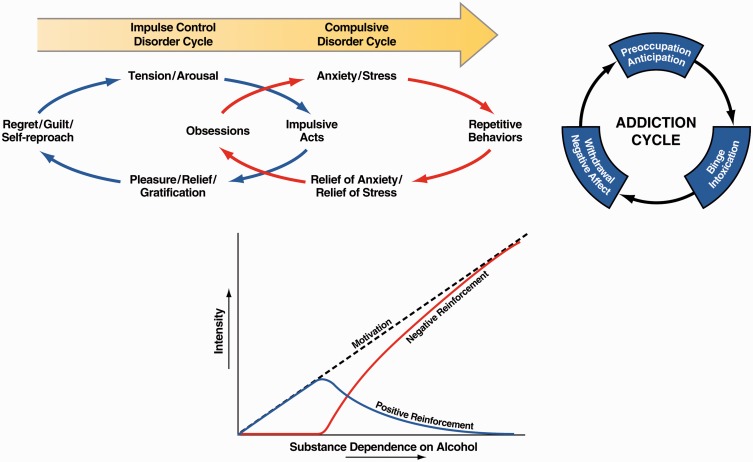
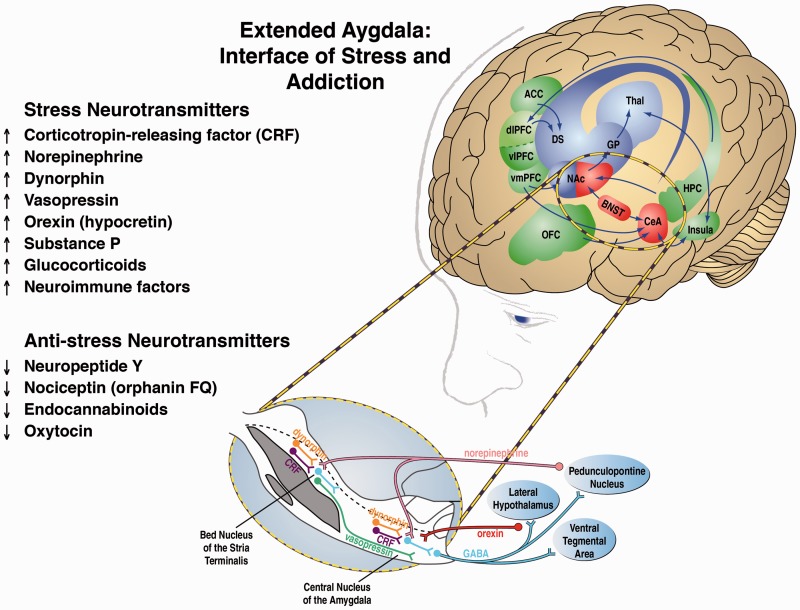
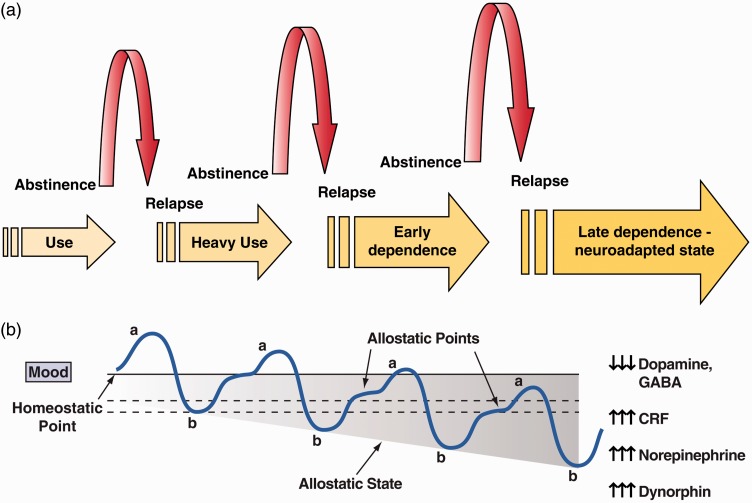
Addiction has been conceptualized as a three-stage cycle-binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation-that worsens over time and involves allostatic changes in hedonic function via changes in the brain reward and stress systems. Using the withdrawal/negative affect stage and negative reinforcement as an important source of motivation for compulsive drug seeking, we outline the neurobiology of the stress component of the withdrawal/negative affect stage and relate it to a derivative of the Research Domain Criteria research construct for the study of psychiatric disease, known as the Addictions Neuroclinical Assessment. Using the Addictions Neuroclinical Assessment, we outline five subdomains of negative emotional states that can be operationally measured in human laboratory settings and paralleled by animal models. We hypothesize that a focus on negative emotionality and stress is closely related to the acute neurobiological alterations that are experienced in addiction and may serve as a bridge to a reformulation of the addiction nosology to better capture individual differences in patients for whom the withdrawal/negative affect stage drives compulsive drug taking.
Keywords: Addiction; alcohol; negative affect; neuroscience; stress.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Selye H. A syndrome produced by diverse nocuous agents. Nature 1936; 138: 32. - PubMed
-
- Burchfield S. The stress response: a new perspective. Psychosom Med 1979; 41: 661–672. - PubMed
-
- Mason JW. A re-evaluation of the concept of “non-specificity” in stress theory. J Psychiatr Res 1971; 8: 323–333. - PubMed
-
- Vale W, Spiess J, Rivier C, et al. Characterization of a 41-residue ovine hypothalamic peptide that stimulates the secretion of corticotropin and -endorphin. Science 1981; 213: 1394–1397. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
