

Cardiac quantitative susceptibility mapping (QSM) for heart chamber oxygenation
- PMID: 28653375
- PMCID: PMC5743772
- DOI: 10.1002/mrm.26808
Cardiac quantitative susceptibility mapping (QSM) for heart chamber oxygenation
Abstract
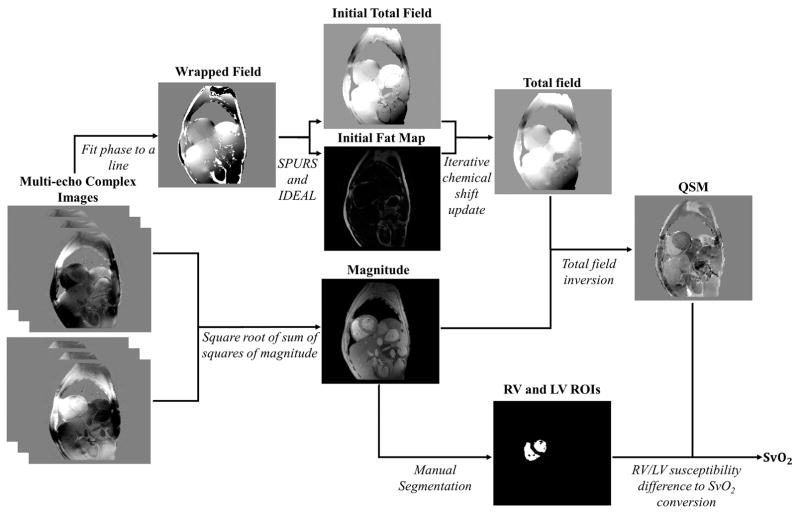
Purpose: To demonstrate the feasibility of in vivo quantitative susceptibility mapping (QSM) in cardiac MRI and to show that mixed-venous oxygen saturation (SvO2 ) can be measured non-invasively using QSM.
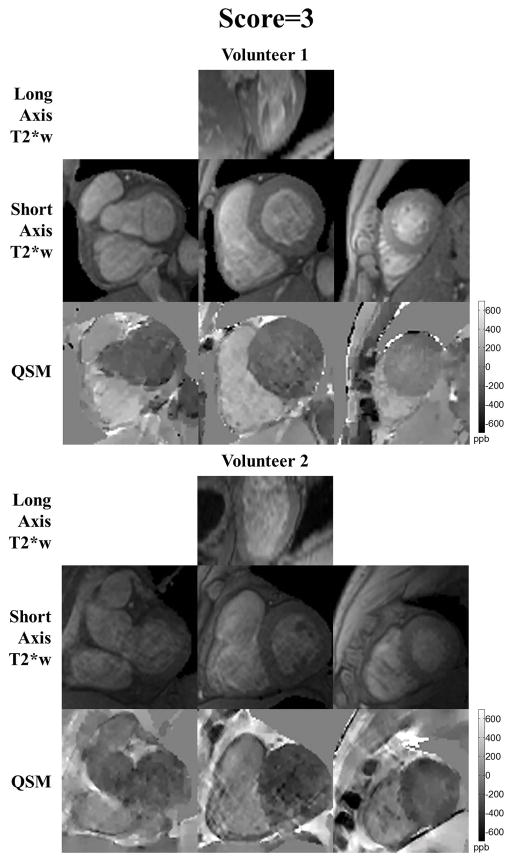
Methods: Electrocardiographic-gated multi-echo 2D gradient echo data were collected at 1.5 T from 14 healthy volunteers during successive breath-holds. Phase wraps and fat chemical shift were removed using a graph-cut-based phase analysis and IDEAL in an iterative approach. The large susceptibility range from air in the lungs to blood in the heart was addressed by using the preconditioning approach in the dipole field inversion. SvO2 was calculated based on the difference in blood susceptibility between the right ventricle (RV) and left ventricle (LV). Cardiac QSM quality was assessed by two independent readers.
Results: Nine out of fourteen volunteers (64%) yielded interpretable cardiac QSM. QSM maps showed strong differential contrast between RV and LV blood with RV blood having higher susceptibility values (291.5 ± 32.4 ppb), which correspond to 78.3 ± 2.3% SvO2 .
Conclusion: In vivo cardiac QSM is feasible and can be used to measure SvO2 , but improvements in data acquisition are needed. Magn Reson Med 79:1545-1552, 2018. © 2017 International Society for Magnetic Resonance in Medicine.
Keywords: cardiac magnetic resonance imaging (cardiac MRI); mixed venous oxygen saturation (SvO2); quantitative susceptibility mapping (QSM).
© 2017 International Society for Magnetic Resonance in Medicine.
Figures



Similar articles
-
Investigating hyperoxic effects in the rat brain using quantitative susceptibility mapping based on MRI phase.Magn Reson Med. 2017 Feb;77(2):592-602. doi: 10.1002/mrm.26139. Epub 2016 Feb 1. Magn Reson Med. 2017. PMID: 26834053
-
Free breathing three-dimensional cardiac quantitative susceptibility mapping for differential cardiac chamber blood oxygenation - initial validation in patients with cardiovascular disease inclusive of direct comparison to invasive catheterization.J Cardiovasc Magn Reson. 2019 Nov 18;21(1):70. doi: 10.1186/s12968-019-0579-7. J Cardiovasc Magn Reson. 2019. PMID: 31735165 Free PMC article.
-
Effect of respiratory hyperoxic challenge on magnetic susceptibility in human brain assessed by quantitative susceptibility mapping (QSM).NMR Biomed. 2015 Dec;28(12):1688-96. doi: 10.1002/nbm.3433. Epub 2015 Oct 20. NMR Biomed. 2015. PMID: 26484968
-
Quantitative susceptibility mapping (QSM): Decoding MRI data for a tissue magnetic biomarker.Magn Reson Med. 2015 Jan;73(1):82-101. doi: 10.1002/mrm.25358. Epub 2014 Jul 17. Magn Reson Med. 2015. PMID: 25044035 Free PMC article. Review.
-
Clinical quantitative susceptibility mapping (QSM): Biometal imaging and its emerging roles in patient care.J Magn Reson Imaging. 2017 Oct;46(4):951-971. doi: 10.1002/jmri.25693. Epub 2017 Mar 10. J Magn Reson Imaging. 2017. PMID: 28295954 Free PMC article. Review.
Cited by
-
Reliable Off-Resonance Correction in High-Field Cardiac MRI Using Autonomous Cardiac B0 Segmentation with Dual-Modality Deep Neural Networks.Bioengineering (Basel). 2024 Feb 23;11(3):210. doi: 10.3390/bioengineering11030210. Bioengineering (Basel). 2024. PMID: 38534485 Free PMC article.
-
Accurate Intramyocardial Hemorrhage Assessment with Fast, Free-running, Cardiac Quantitative Susceptibility Mapping.Radiol Cardiothorac Imaging. 2024 Dec;6(6):e230376. doi: 10.1148/ryct.230376. Radiol Cardiothorac Imaging. 2024. PMID: 39665631 Free PMC article.
-
Trajectory correction enables free-running chemical shift encoded imaging for accurate cardiac proton-density fat fraction quantification at 3T.J Cardiovasc Magn Reson. 2024 Winter;26(2):101048. doi: 10.1016/j.jocmr.2024.101048. Epub 2024 Jun 13. J Cardiovasc Magn Reson. 2024. PMID: 38878970 Free PMC article.
-
QSM Throughout the Body.J Magn Reson Imaging. 2023 Jun;57(6):1621-1640. doi: 10.1002/jmri.28624. Epub 2023 Feb 7. J Magn Reson Imaging. 2023. PMID: 36748806 Free PMC article. Review.
-
LARO: Learned acquisition and reconstruction optimization to accelerate quantitative susceptibility mapping.Neuroimage. 2023 Mar;268:119886. doi: 10.1016/j.neuroimage.2023.119886. Epub 2023 Jan 17. Neuroimage. 2023. PMID: 36669747 Free PMC article.
References
-
- Brovman EY, Gabriel RA, Dutton RP, Urman RD. Pulmonary Artery Catheter Use During Cardiac Surgery in the United States, 2010 to 2014. Journal of Cardiothoracic and Vascular Anesthesia. 2016;30(3):579–584. - PubMed
-
- Judge O, Ji F, Fleming N, Liu H. Current Use of the Pulmonary Artery Catheter in Cardiac Surgery: A Survey Study. Journal of Cardiothoracic and Vascular Anesthesia. 2015;29(1):69–75. - PubMed
-
- Jesurum J. Svo2 Monitoring. Critical Care Nurse. 2004;24(4):73–76.
-
- Nield LE, Qi X-LL, Valsangiacomo ER, Macgowan CK, Wright GA, Hornberger LK, Yoo S-J. In vivo MRI measurement of blood oxygen saturation in children with congenital heart disease. Pediatric Radiology. 2005;35(2):179–185. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
