

Risk factors for cryptorchidism
- PMID: 28654092
- PMCID: PMC5815831
- DOI: 10.1038/nrurol.2017.90
Risk factors for cryptorchidism
Abstract
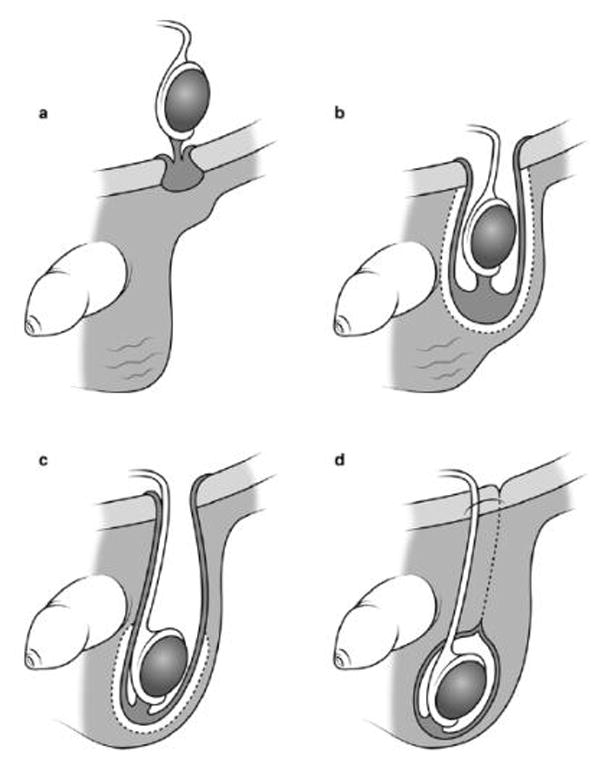
Undescended testis - known as cryptorchidism - is one of the most common congenital abnormalities observed in boys, and is one of the few known risk factors for testicular cancer. The key factors that contribute to the occurrence of cryptorchidism remain elusive. Testicular descent is thought to occur during two hormonally-controlled phases in fetal development - between 8-15 weeks (the first phase of decent) and 25-35 weeks gestation (the second phase of descent); the failure of a testis to descend permanently is probably caused by disruptions to one or both of these phases, but the causes and mechanisms of such disruptions are still unclear. A broad range of putative risk factors have been evaluated in relation to the development of cryptorchidism but their plausibility is still in question. Consistent evidence of an association with cryptorchidism exists for only a few factors, and in those cases in which evidence seems unequivocal the factor is likely to be a surrogate for the true causal exposure. The relative importance of each risk factor could vary considerably between mother-son pairs depending on an array of genetic, maternal, placental and fetal factors - all of which could vary between regions. Thus, the role of causative factors in aetiology of cryptorchidism requires further research.
Figures
References
-
- Berkowitz GS, et al. Prevalence and natural history of cryptorchidism. Pediatrics. 1993;92:44–49. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
