

Effect of Electronic Reminders, Financial Incentives, and Social Support on Outcomes After Myocardial Infarction: The HeartStrong Randomized Clinical Trial
- PMID: 28654972
- PMCID: PMC5710431
- DOI: 10.1001/jamainternmed.2017.2449
Effect of Electronic Reminders, Financial Incentives, and Social Support on Outcomes After Myocardial Infarction: The HeartStrong Randomized Clinical Trial
Abstract
Importance: Adherence to medications prescribed after acute myocardial infarction (AMI) is low. Wireless technology and behavioral economic approaches have shown promise in improving health behaviors.
Objective: To determine whether a system of medication reminders using financial incentives and social support delays subsequent vascular events in patients following AMI compared with usual care.
Design, setting, and participants: Two-arm, randomized clinical trial with a 12-month intervention conducted from 2013 through 2016. Investigators were blinded to study group, but participants were not. Design was a health plan-intermediated intervention for members of several health plans. We recruited 1509 participants from 7179 contacted AMI survivors (insured with 5 large US insurers nationally or with Medicare fee-for-service at the University of Pennsylvania Health System). Patients aged 18 to 80 years were eligible if currently prescribed at least 2 of 4 study medications (statin, aspirin, β-blocker, antiplatelet agent), and were hospital inpatients for 1 to 180 days and discharged home with a principal diagnosis of AMI.
Interventions: Patients were randomized 2:1 to an intervention using electronic pill bottles combined with lottery incentives and social support for medication adherence (1003 patients), or to usual care (506 patients).
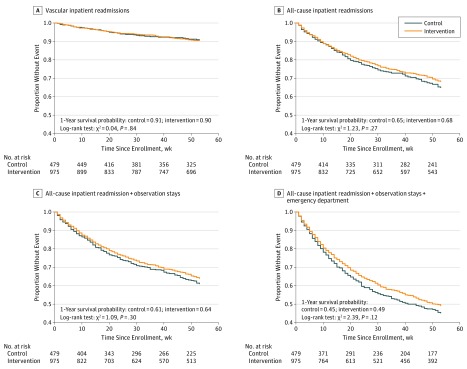
Main outcomes and measures: Primary outcome was time to first vascular rehospitalization or death. Secondary outcomes were time to first all-cause rehospitalization, total number of repeated hospitalizations, medication adherence, and total medical costs.
Results: A total of 35.5% of participants were female (n = 536); mean (SD) age was 61.0 (10.3) years. There were no statistically significant differences between study arms in time to first rehospitalization for a vascular event or death (hazard ratio, 1.04; 95% CI, 0.71 to 1.52; P = .84), time to first all-cause rehospitalization (hazard ratio, 0.89; 95% CI, 0.73 to 1.09; P = .27), or total number of repeated hospitalizations (hazard ratio, 0.94; 95% CI, 0.60 to 1.48; P = .79). Mean (SD) medication adherence did not differ between control (0.42 [0.39]) and intervention (0.46 [0.39]) (difference, 0.04; 95% CI, -0.01 to 0.09; P = .10). Mean (SD) medical costs in 12 months following enrollment did not differ between control ($29 811 [$74 850]) and intervention ($24 038 [$66 915]) (difference, -$5773; 95% CI, -$13 682 to $2137; P = .15).
Conclusions and relevance: A compound intervention integrating wireless pill bottles, lottery-based incentives, and social support did not significantly improve medication adherence or vascular readmission outcomes for AMI survivors.
Trial registration: clinicaltrials.gov Identifier: NCT01800201.
Conflict of interest statement
Figures

References
-
- Choudhry NK, Avorn J, Glynn RJ, et al. ; Post-Myocardial Infarction Free Rx Event and Economic Evaluation (MI FREEE) Trial . Full coverage for preventive medications after myocardial infarction. N Engl J Med. 2011;365(22):2088-2097. - PubMed
-
- Loewenstein G, Asch DA, Volpp KG. Behavioral economics holds potential to deliver better results for patients, insurers, and employers. Health Aff (Millwood). 2013;32(7):1244-1250. - PubMed
-
- Asch DA, Muller RW, Volpp KG. Automated hovering in health care—watching over the 5000 hours. N Engl J Med. 2012;367(1):1-3. - PubMed
-
- Troxel AB, Asch DA, Mehta SJ, et al. Rationale and design of a randomized trial of automated hovering for post-myocardial infarction patients: the HeartStrong program. Am Heart J. 2016;179:166-174. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
