

Evaluating Surgeon-Specific Performance for Endoscopic Sinus Surgery
- PMID: 28655057
- PMCID: PMC5710289
- DOI: 10.1001/jamaoto.2017.0752
Evaluating Surgeon-Specific Performance for Endoscopic Sinus Surgery
Abstract
Importance: Several identified factors have raised questions concerning the quality of care for endoscopic sinus surgery (ESS), including the presence of large geographic variation in the rates and extent of surgery, poorly defined indications, and lack of ESS-specific quality metrics. Combined with the risk of major complications, ESS represents a high-value target for quality improvement.
Objective: To evaluate differences in surgeon-specific performance for ESS using a risk-adjusted, 5-year ESS revision rate as a quality metric.
Design, setting, and participants: This retrospective study used a population-based administrative database to study adults (≥18 years of age) with chronic rhinosinusitis (CRS) who underwent primary ESS in Alberta, Canada, between March 1, 2007, and March 1, 2010. The study period ended in 2015 to provide 5 years of follow-up.
Interventions: Endoscopic sinus surgery for CRS.
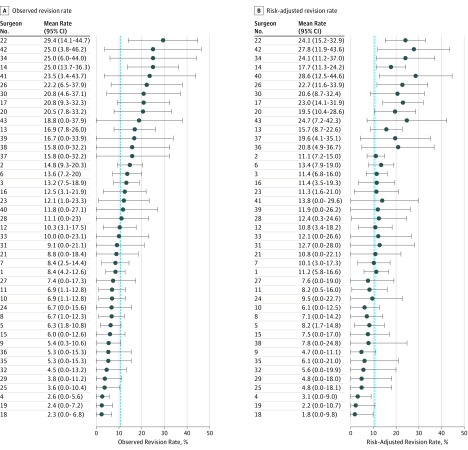
Main outcomes and measures: Primary outcomes were the 5-year observed and risk-adjusted ESS revision rate. Logistic regression was used to develop a risk adjustment model for the primary outcome.
Results: A total of 43 individual surgeons performed primary ESS in 2168 patients with CRS. Within 5 years after the primary ESS procedure, 239 patients underwent revision ESS, and the mean crude 5-year ESS revision rate was 10.6% (range, 2.4%-28.6%). After applying the risk adjustment model and 95% CI to each surgeon, 7 surgeons (16%) had lower-than-expected performance and 2 surgeons (5%) had higher-than-expected performance. Three variables had significant associations with surgeon-specific, 5-year ESS revision rates: presence of nasal polyps (odds ratio [OR], 2.07; 95% CI, 1.59-2.70), more annual systemic corticosteroid courses (OR, 1.33; 95% CI, 1.19-1.48), and concurrent septoplasty (OR, 0.70; 95% CI, 0.55-0.89).
Conclusions and relevance: Evaluating surgeon-specific performance for ESS may provide information to assist in quality improvement. Although most surgeons had comparable risk-adjusted, 5-year ESS revision rates, 16% of surgeons had lower-than-expected performance, indicating a potential to improve quality of care. Future studies are needed to evaluate more surgeon-specific variables and validate a risk adjustment model to provide appropriate feedback for quality improvement.
Conflict of interest statement
Figures
Similar articles
-
Revision endoscopic sinus surgery rates by chronic rhinosinusitis subtype.Int Forum Allergy Rhinol. 2018 Sep;8(9):1047-1051. doi: 10.1002/alr.22146. Epub 2018 May 31. Int Forum Allergy Rhinol. 2018. PMID: 29851243
-
Regional differences in endoscopic sinus surgery in Finland: a nationwide register-based study.BMJ Open. 2018 Oct 18;8(10):e022173. doi: 10.1136/bmjopen-2018-022173. BMJ Open. 2018. PMID: 30341122 Free PMC article.
-
Defining appropriateness criteria for endoscopic sinus surgery during management of uncomplicated adult chronic rhinosinusitis: a RAND/UCLA appropriateness study.Int Forum Allergy Rhinol. 2016 Jun;6(6):557-67. doi: 10.1002/alr.21769. Epub 2016 Mar 11. Int Forum Allergy Rhinol. 2016. PMID: 26970538
-
Revision surgery rates in chronic rhinosinusitis with nasal polyps: meta-analysis of risk factors.Int Forum Allergy Rhinol. 2020 Feb;10(2):199-207. doi: 10.1002/alr.22487. Epub 2019 Nov 21. Int Forum Allergy Rhinol. 2020. PMID: 31752051
-
Contemporary considerations in concurrent endoscopic sinus surgery and rhinoplasty.Curr Opin Otolaryngol Head Neck Surg. 2018 Aug;26(4):209-213. doi: 10.1097/MOO.0000000000000469. Curr Opin Otolaryngol Head Neck Surg. 2018. PMID: 29894317 Review.
Cited by
-
Is There a Surgeons' Effect on Patients' Physical Health, Beyond the Intervention, That Requires Further Investigation? A Systematic Review.Ther Clin Risk Manag. 2022 Apr 26;18:467-490. doi: 10.2147/TCRM.S357934. eCollection 2022. Ther Clin Risk Manag. 2022. PMID: 35502434 Free PMC article. Review.
-
Characteristics of Exceptionally Good Doctors: A Protocol for a Cross-Sectional Survey of Adults.Patient Relat Outcome Meas. 2022 Aug 12;13:181-188. doi: 10.2147/PROM.S376033. eCollection 2022. Patient Relat Outcome Meas. 2022. PMID: 35983576 Free PMC article.
-
Qualitative Study of Medical Doctors on Their Experiences and Opinions of the Characteristics of Exceptionally Good Doctors.Adv Med Educ Pract. 2022 Jul 17;13:717-731. doi: 10.2147/AMEP.S370980. eCollection 2022. Adv Med Educ Pract. 2022. PMID: 35872967 Free PMC article.
-
THE 2017 13TH ANNUAL DAVID W. KENNEDY, MD, LECTURE The evolution of outcomes in sinus surgery for chronic rhinosinusitis: past, present, and future.Int Forum Allergy Rhinol. 2017 Dec;7(12):1121-1126. doi: 10.1002/alr.22026. Epub 2017 Oct 13. Int Forum Allergy Rhinol. 2017. PMID: 29028274 Free PMC article.
-
The Doctors' Effect on Patients' Physical Health Outcomes Beyond the Intervention: A Methodological Review.Clin Epidemiol. 2022 Jul 18;14:851-870. doi: 10.2147/CLEP.S357927. eCollection 2022. Clin Epidemiol. 2022. PMID: 35879943 Free PMC article.
References
-
- Duclos A, Carty MJ. Value of health care delivery. JAMA. 2011;306(3):267. - PubMed
-
- Kaplan RS, Porter ME. How to solve the cost crisis in health care. Harv Bus Rev. 2011;89(9):46-52, 54, 56-61 passim. - PubMed
-
- Blumenthal D. Better health care: a way forward. JAMA. 2016;315(13):1333-1334. - PubMed
-
- Dimick JB, Weeks WB, Karia RJ, Das S, Campbell DA Jr. Who pays for poor surgical quality? building a business case for quality improvement. J Am Coll Surg. 2006;202(6):933-937. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
