

Diagnostic delay for giant cell arteritis - a systematic review and meta-analysis
- PMID: 28655311
- PMCID: PMC5488376
- DOI: 10.1186/s12916-017-0871-z
Diagnostic delay for giant cell arteritis - a systematic review and meta-analysis
Abstract
Background: Giant cell arteritis (GCA), if untreated, can lead to blindness and stroke. The study's objectives were to (1) determine a new evidence-based benchmark of the extent of diagnostic delay for GCA and (2) examine the role of GCA-specific characteristics on diagnostic delay.
Methods: Medical literature databases were searched from inception to November 2015. Articles were included if reporting a time-period of diagnostic delay between onset of GCA symptoms and diagnosis. Two reviewers assessed the quality of the final articles and extracted data from these. Random-effects meta-analysis was used to pool the mean time-period (95% confidence interval (CI)) between GCA symptom onset and diagnosis, and the delay observed for GCA-specific characteristics. Heterogeneity was assessed by I 2 and by 95% prediction interval (PI).
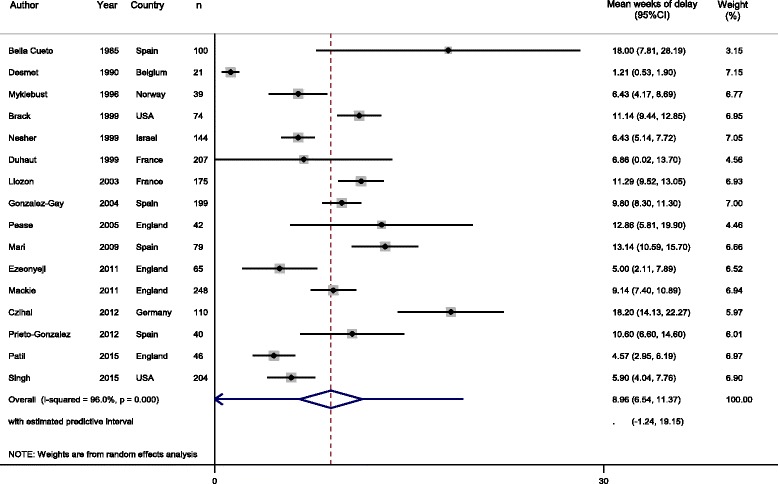
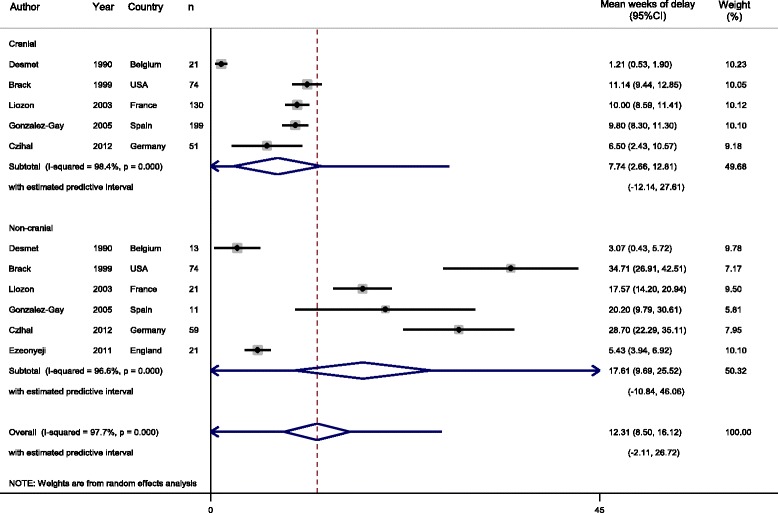
Results: Of 4128 articles initially identified, 16 provided data for meta-analysis. Mean diagnostic delay was 9.0 weeks (95% CI, 6.5 to 11.4) between symptom onset and GCA diagnosis (I 2 = 96.0%; P < 0.001; 95% PI, 0 to 19.2 weeks). Patients with a cranial presentation of GCA received a diagnosis after 7.7 (95% CI, 2.7 to 12.8) weeks (I 2 = 98.4%; P < 0.001; 95% PI, 0 to 27.6 weeks) and those with non-cranial GCA after 17.6 (95% CI, 9.7 to 25.5) weeks (I 2 = 96.6%; P < 0.001; 95% PI, 0 to 46.1 weeks).
Conclusions: The mean delay from symptom onset to GCA diagnosis was 9 weeks, or longer when cranial symptoms were absent. Our research provides an evidence-based benchmark for diagnostic delay of GCA and supports the need for improved public awareness and fast-track diagnostic pathways.
Keywords: Diagnostic delay; Giant cell arteritis; Meta-analysis; Systematic review.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
