

Ultrasonography helps emergency physician identify the best lumbar puncture site under the conus medullaris
- PMID: 28655356
- PMCID: PMC5488483
- DOI: 10.1186/s13049-017-0406-9
Ultrasonography helps emergency physician identify the best lumbar puncture site under the conus medullaris
Abstract
Background: Ultrasonography - assisted lumbar puncture helps physicians identify traditional anatomical landmarks. However, it could help to overcome the anatomical dogmas and thus identify the best interspinous space under the medullary cone.
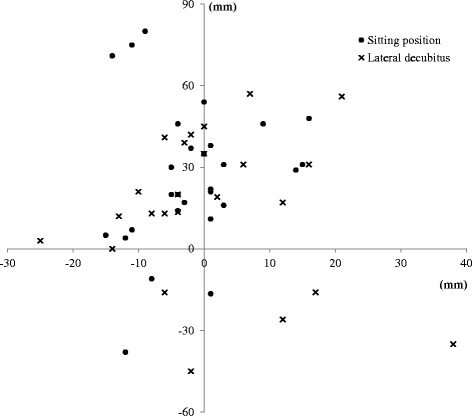
Methods: Traditional anatomical landmarks were reported on a tracing paper in patients with an indication for lumbar puncture. Then, ultrasonography was used to locate the optimal interspinous level defined as the widest subarachnoid space located below the conus medullaris. Primary endpoint was the distance between traditional and ultrasound landmarks.
Results: Fifty-seven patients were included. Seven emergency physicians practiced the procedure. The median absolute distance between traditional anatomical landmarks and ultrasound marking was 32 [interquartile (IQR) 27 - 37] mm. The inter-spinous space identified in the two procedures was different in 68% of the cases.
Conclusions: Ultrasound not only allows us to better identify anatomical structures before lumbar puncture, but it also allows us to choose a site of puncture different from recommendations.
Keywords: Emergency; Lumbar puncture; Ultrasonography.
Figures
Comment in
-
Proper training and use of ultrasonography facilitates lumbar puncture.Scand J Trauma Resusc Emerg Med. 2017 Dec 20;25(1):121. doi: 10.1186/s13049-017-0466-x. Scand J Trauma Resusc Emerg Med. 2017. PMID: 29262853 Free PMC article.
References
-
- Neal JT, Kaplan SL, Woodford AL, Desai K, Zorc JJ, Chen AE. The Effect of Bedside Ultrasonographic Skin Marking on Infant Lumbar Puncture Success: A Randomized Controlled Trial. Ann Emerg Med. 2017;69(5):610–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
