

National Differences in Trends for Heart Failure Hospitalizations by Sex and Race/Ethnicity
- PMID: 28655709
- PMCID: PMC5540644
- DOI: 10.1161/CIRCOUTCOMES.116.003552
National Differences in Trends for Heart Failure Hospitalizations by Sex and Race/Ethnicity
Abstract
Background: National heart failure (HF) hospitalization rates have not been appropriately age standardized by sex or race/ethnicity. Reporting hospital utilization trends by subgroup is important for monitoring population health and developing interventions to eliminate disparities.
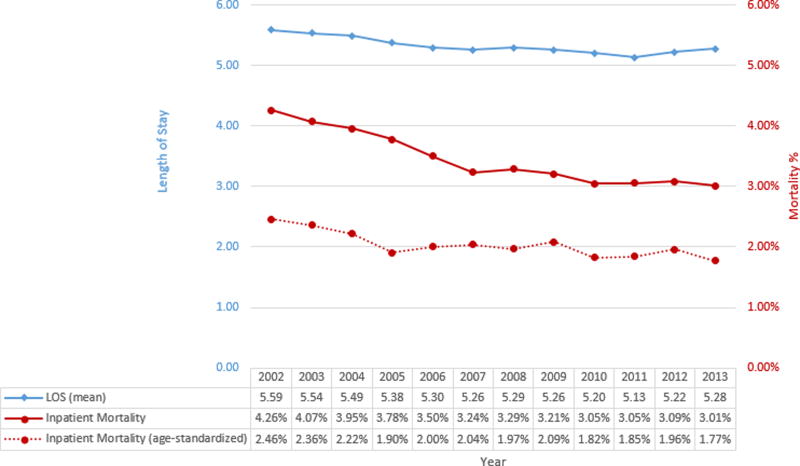
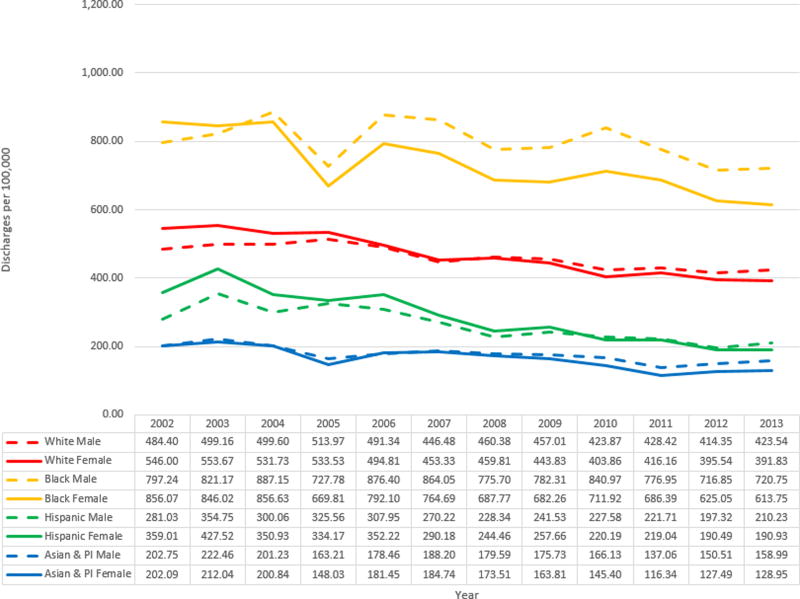
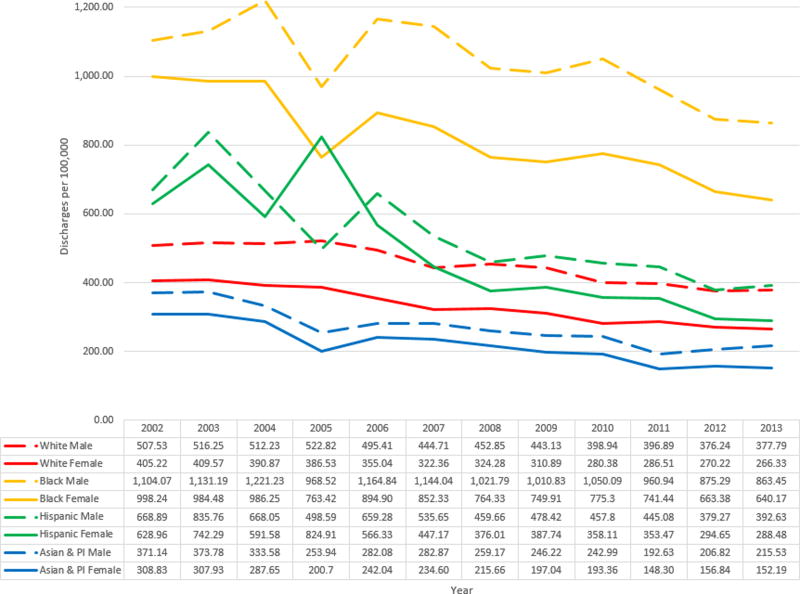
Methods and results: The National Inpatient Sample (NIS) was used to estimate the crude and age-standardized rates of HF hospitalization between 2002 and 2013 by sex and race/ethnicity. Direct standardization was used to age-standardize rates to the 2000 US standard population. Relative differences between subgroups were reported. The national age-adjusted HF hospitalization rate decreased 30.8% from 526.86 to 364.66 per 100 000 between 2002 and 2013. Although hospitalizations decreased for all subgroups, the ratio of the age-standardized rate for men compared with women increased from 20% greater to 39% (P trend=0.002) between 2002 and 2013. Black men had a rate that was 229% (P trend=0.141) and black women, 240% (P trend=0.725) with reference to whites in 2013 with no significant change between 2002 and 2013. Hispanic men had a rate that was 32% greater in 2002 and the difference narrowed to 4% (P trend=0.047) greater in 2013 relative to whites. For Hispanic women, the rate was 55% greater in 2002 and narrowed to 8% greater (P trend=0.004) in 2013 relative to whites. Asian/Pacific Islander men had a 27% lower rate in 2002 that improved to 43% (P trend=0.040) lower in 2013 relative to whites. For Asian/Pacific Islander women, the hospitalization rate was 24% lower in 2002 and improved to 43% (P trend=0.021) lower in 2013 relative to whites.
Conclusions: National HF hospitalization rates have decreased steadily during the recent decade. Disparities in HF burden and hospital utilization by sex and race/ethnicity persist. Significant population health interventions are needed to reduce the HF hospitalization burden among blacks. An evaluation of factors explaining the improvements in the HF hospitalization rates among Hispanics and Asian/Pacific Islanders is needed.
Keywords: comorbidity; healthcare disparities; heart failure; hospitalization; population groups; population surveillance; public health.
© 2017 American Heart Association, Inc.
Figures
References
-
- Pfuntner A, Wier LM, Stocks C. Most Frequent Conditions in U.S. Hospitals, 2011. Rockville, Maryland: 2013. Available from: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb162.jsp. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després J-P, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jiménez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133:e38–e360. - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Piña IL, Trogdon JG. Forecasting the impact of heart failure in the united states a policy statement from the american heart association. Circ Heart Fail. 2013;6:606–619. - PMC - PubMed
-
- Okura Y, Urban LH, Mahoney DW, Jacobsen SJ, Rodeheffer RJ. Agreement between self-report questionnaires and medical record data was substantial for diabetes, hypertension, myocardial infarction and stroke but not for heart failure. J Clin Epidemiol. 2004;57:1096–1103. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
