

Difficult Laparoscopic Cholecystectomy and Trainees: Predictors and Results in an Academic Teaching Hospital
- PMID: 28656045
- PMCID: PMC5474555
- DOI: 10.1155/2017/6467814
Difficult Laparoscopic Cholecystectomy and Trainees: Predictors and Results in an Academic Teaching Hospital
Abstract
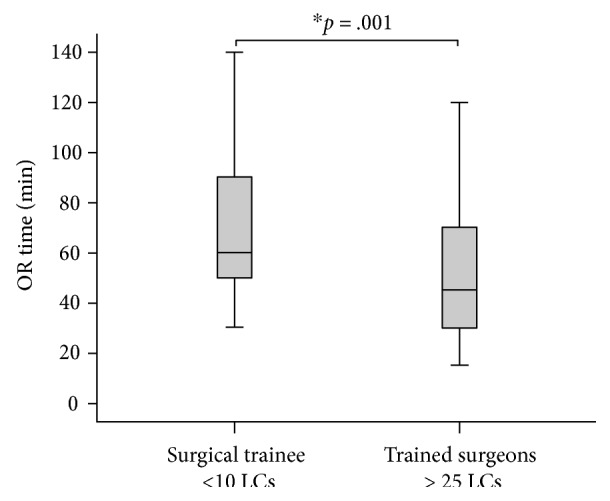
Laparoscopic cholecystectomy (LC) is one of the first laparoscopic procedures performed by surgical trainees. This study aims to determine preoperative and/or intraoperative predictors of difficult LC and to compare complications of LC performed by trainees with that performed by trained surgeons. A cohort of 180 consecutive patients with cholelithiasis who underwent LC was analyzed. We used univariate and binary logistic regression analyses to predict factors associated with difficult LC. We compared the rate of complications of LCs performed by trainees and that performed by trained surgeons using Pearson's chi-square test. Patients with impacted stone in the neck of the gallbladder (GB) (OR, 5.0; 95% CI, 1.59-15.77), with adhesions in the Triangle of Calot (OR, 2.9; 95% CI, 1.27-6.83), or with GB rupture (OR, 3.4; 95% CI, 1.02-11.41) were more likely to experience difficult LC. There was no difference between trainees and trained surgeons in the rate of cystic artery injury (p = .144) or GB rupture (p = .097). However, operative time of LCs performed by trained surgeons was significantly shorter (median, 45 min; IQR, 30-70 min) compared with the surgical trainees' operative time (60 min; IQR, 50-90 min). Surgical trainees can perform difficult LC safely under supervision with no increase in complications albeit with mild increase in operative time.
Figures
References
-
- Keus F., Gooszen H. G., van Laarhoven C. J. Open, small-incision, or laparoscopic cholecystectomy for patients with symptomatic cholecystolithiasis. An overview of Cochrane Hepato-Biliary Group reviews. The Cochrane Database of Systematic Reviews. 2010;(1, article CD008318) doi: 10.1002/14651858.CD008318. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
