

Toxins in Brain! Magnetic Resonance (MR) Imaging of Toxic Leukoencephalopathy - A Pictorial Essay
- PMID: 28656068
- PMCID: PMC5478246
- DOI: 10.12659/PJR.901791
Toxins in Brain! Magnetic Resonance (MR) Imaging of Toxic Leukoencephalopathy - A Pictorial Essay
Abstract
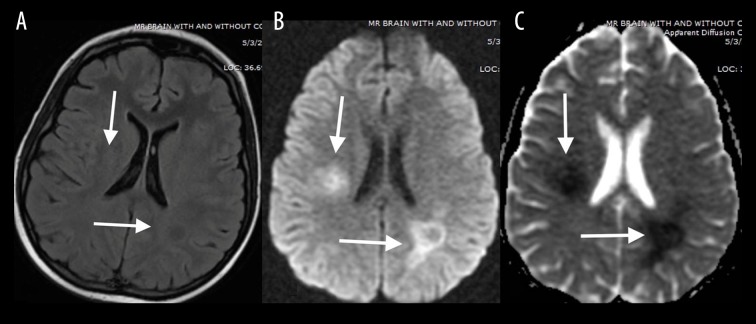
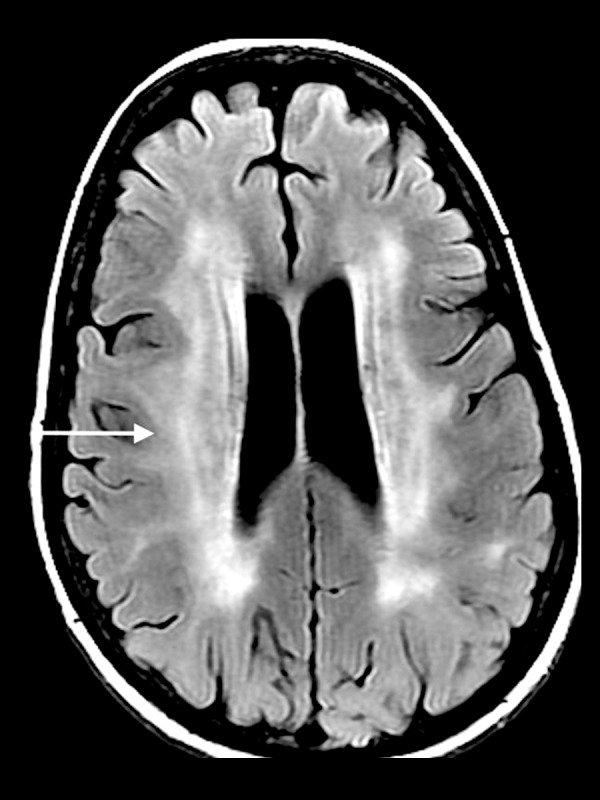
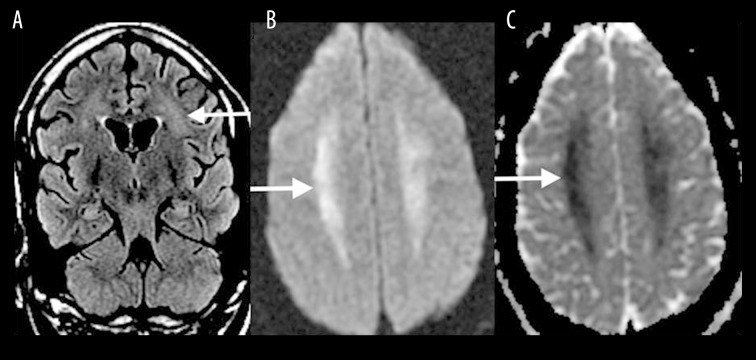
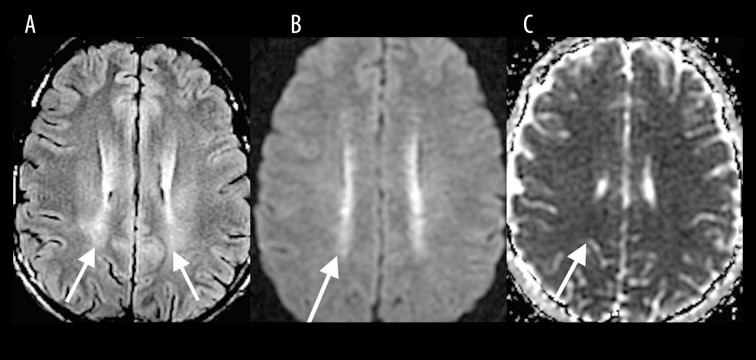
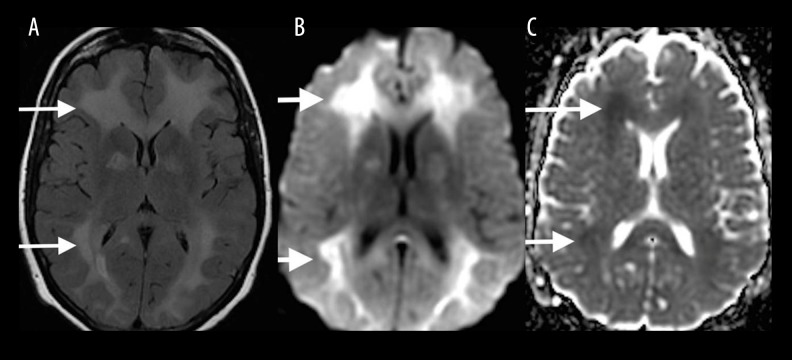
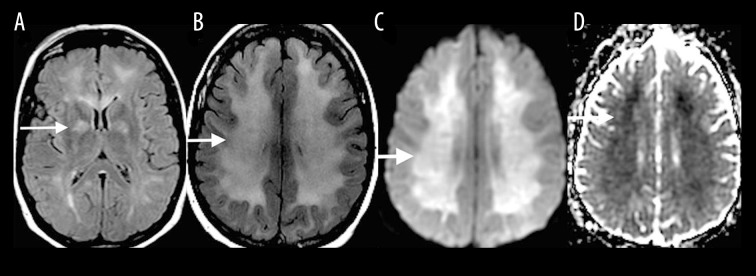
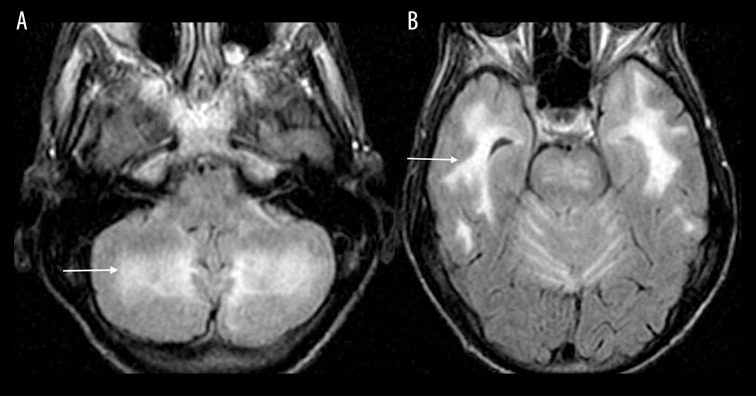
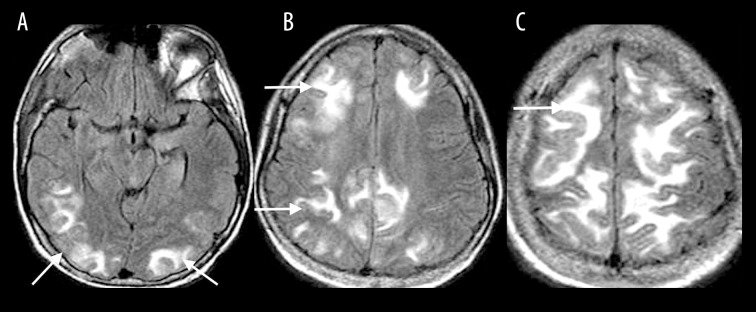
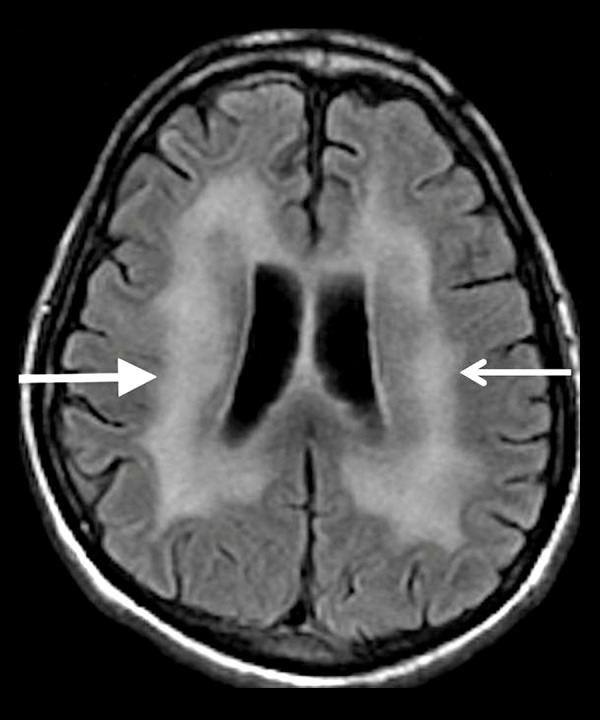
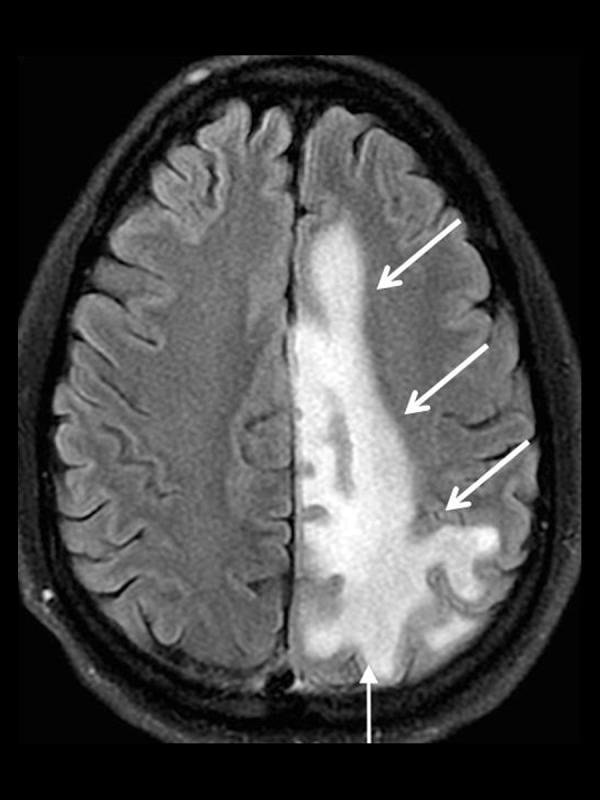
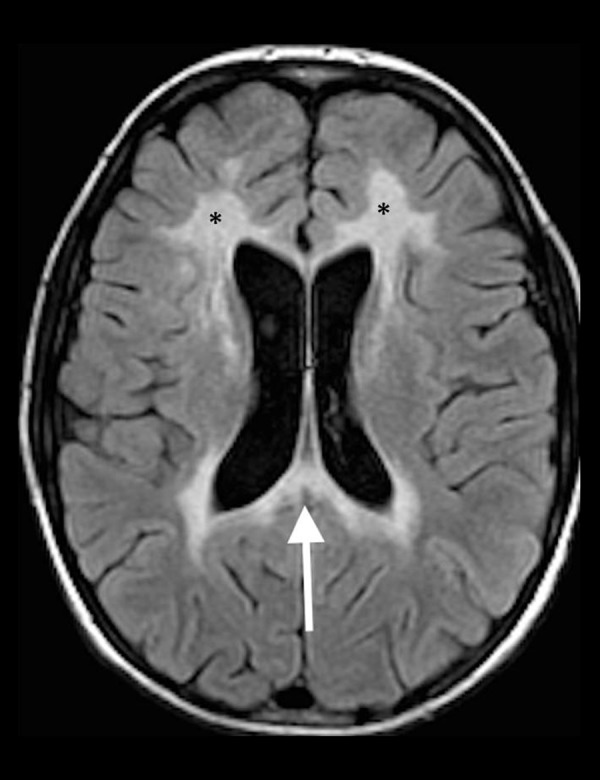
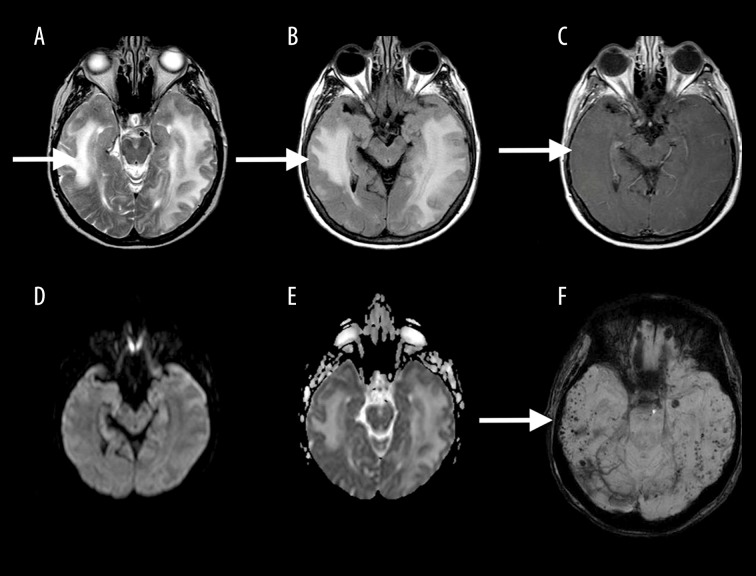
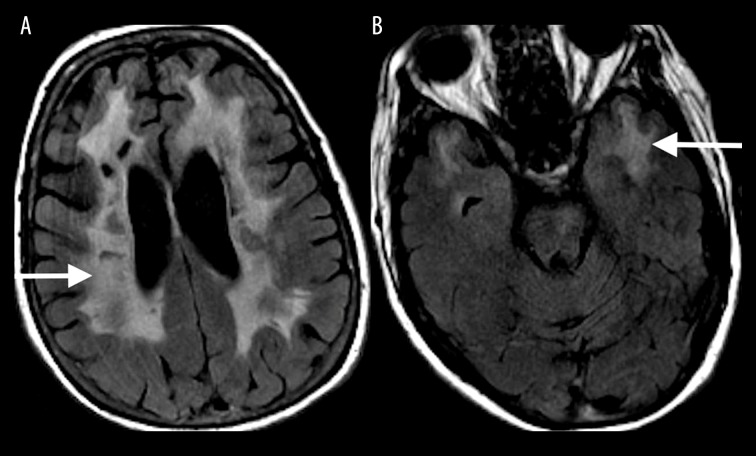
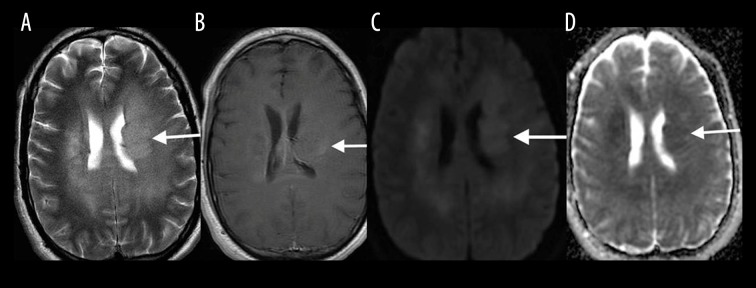
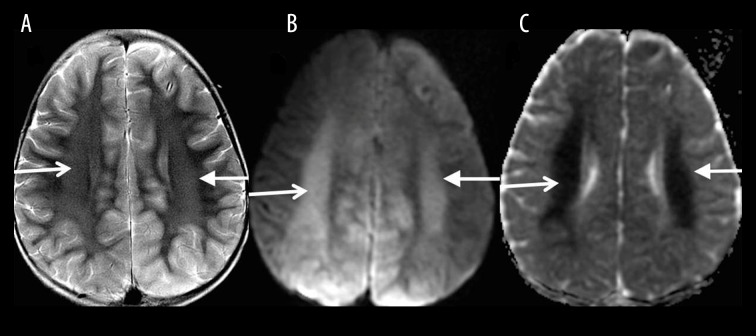
Toxic leukoencephalopathy results from damage to the white matter caused by various toxins. It manifests itself as white matter signal abnormalities with or without the presence of restricted diffusion. These changes are often reversible if the insulting agent is removed early, with the exception of posthypoxic leukoencephalopathy that can manifest itself 1-2 weeks after the initial insult. However, many other potential causes of white matter signal abnormalities can mimic the changes of toxic leukoencephalopathy. Thus, familiarity with the causes, clinical presentation and particularly imaging findings of toxic leukoencephalopathy is critical for early treatment and improved prognosis. The purpose of this pictorial essay is to familiarize the reader with the various causes of toxic leukoencephalopathy along with its differential diagnoses and mimics.
Keywords: Brain Diseases, Metabolic; Magnetic Resonance Imaging; Toxic Actions.
Conflict of interest statement
Conflict of interest The authors declare that they have no conflict of interest.
Figures

References
-
- Vázquez E, Delgado I, Sánchez-Montañez A, et al. Side effects of oncologic therapies in the pediatric central nervous system: Update on neuroimaging findings. Radiographics. 2011;31:1123–39. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources