

Malignancy Detection on Mammography Using Dual Deep Convolutional Neural Networks and Genetically Discovered False Color Input Enhancement
- PMID: 28656455
- PMCID: PMC5537100
- DOI: 10.1007/s10278-017-9993-2
Malignancy Detection on Mammography Using Dual Deep Convolutional Neural Networks and Genetically Discovered False Color Input Enhancement
Abstract
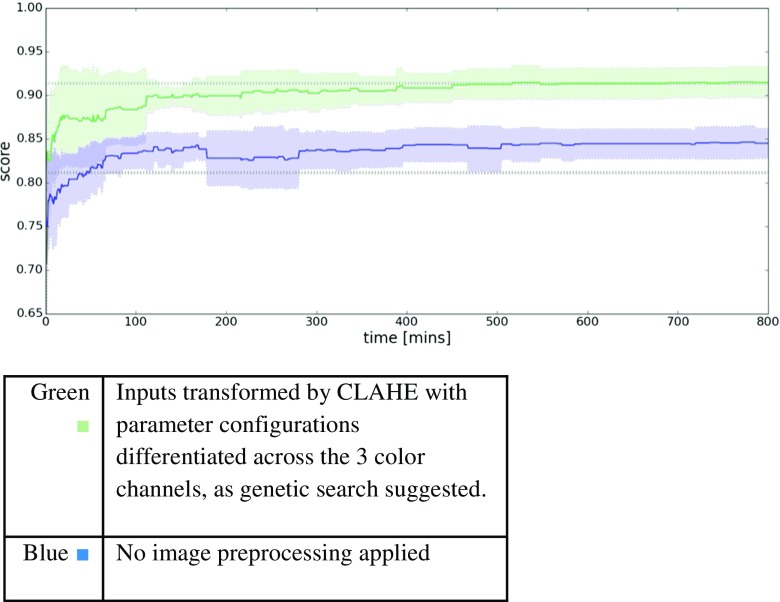
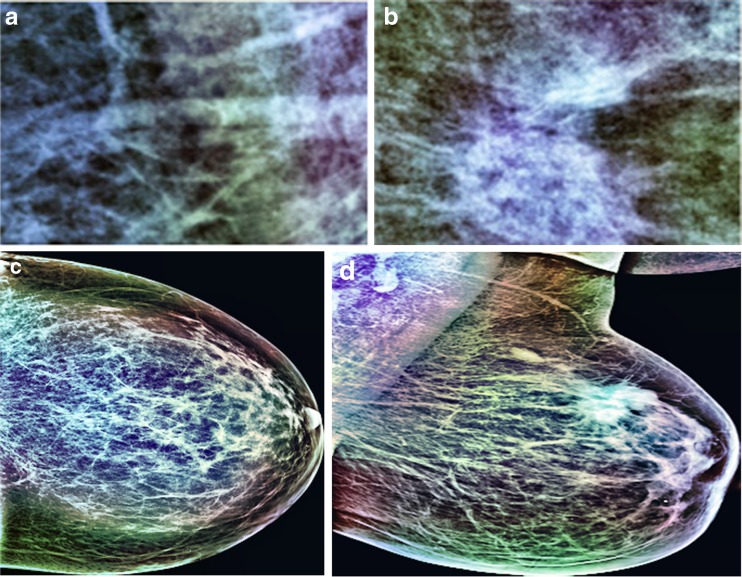
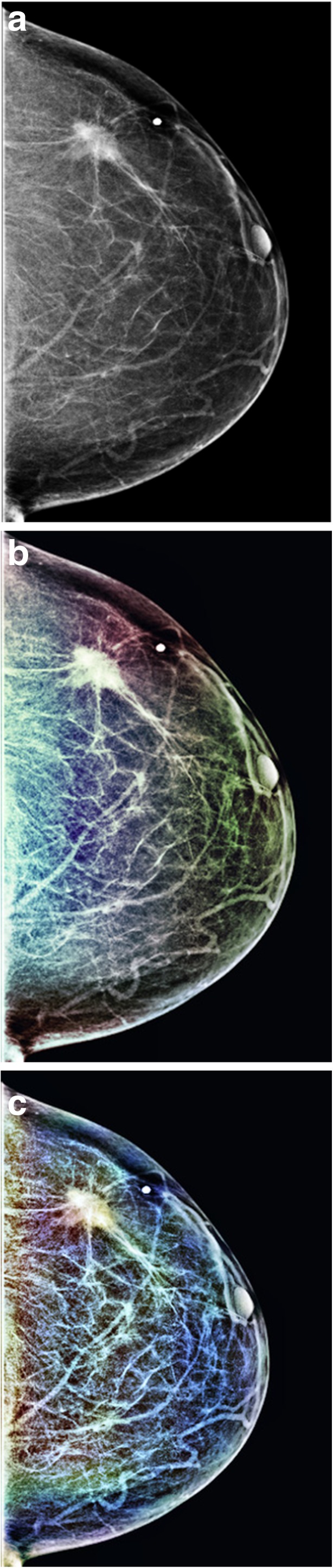
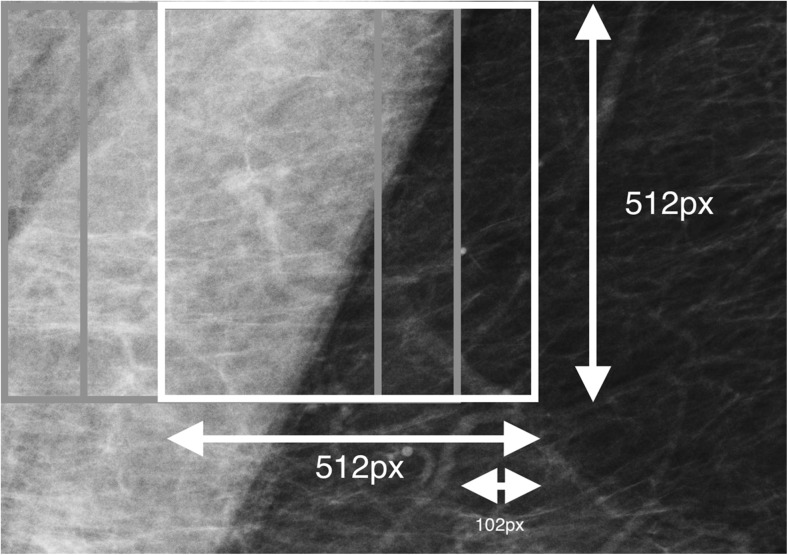
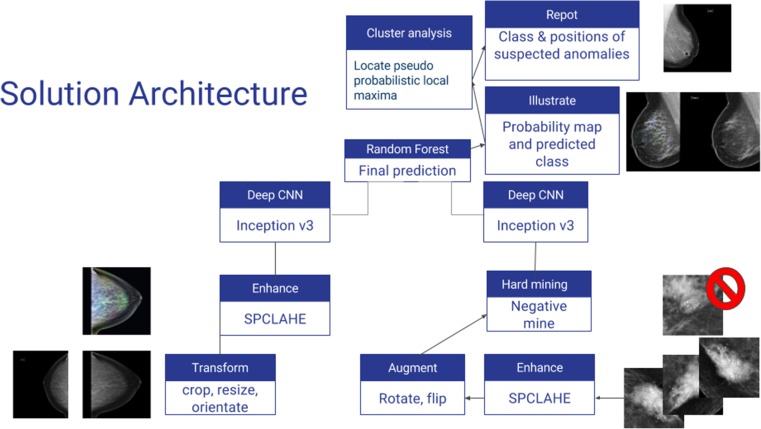
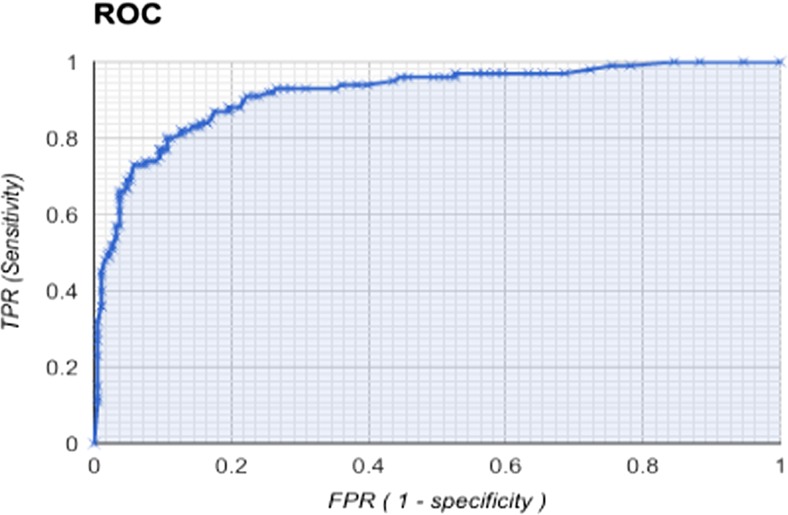
Breast cancer is the most prevalent malignancy in the US and the third highest cause of cancer-related mortality worldwide. Regular mammography screening has been attributed with doubling the rate of early cancer detection over the past three decades, yet estimates of mammographic accuracy in the hands of experienced radiologists remain suboptimal with sensitivity ranging from 62 to 87% and specificity from 75 to 91%. Advances in machine learning (ML) in recent years have demonstrated capabilities of image analysis which often surpass those of human observers. Here we present two novel techniques to address inherent challenges in the application of ML to the domain of mammography. We describe the use of genetic search of image enhancement methods, leading us to the use of a novel form of false color enhancement through contrast limited adaptive histogram equalization (CLAHE), as a method to optimize mammographic feature representation. We also utilize dual deep convolutional neural networks at different scales, for classification of full mammogram images and derivative patches combined with a random forest gating network as a novel architectural solution capable of discerning malignancy with a specificity of 0.91 and a specificity of 0.80. To our knowledge, this represents the first automatic stand-alone mammography malignancy detection algorithm with sensitivity and specificity performance similar to that of expert radiologists.
Keywords: Convolutional neural networks; Deep learning; Machine learning; Mammography.
Conflict of interest statement
Philip Teare, Eyal Toledano, and Eldad Elnekave are employees of Zebra Medical Vision.
Oshra Benzaquen has no conflicts of interest to disclose.
Figures

References
-
- American Cancer Society Cancer Facts & Figures 2015. Cancer Facts Fig. 2015;2015:1–9.
-
- Tabar L, Vitak B, Chen T, Yen A, Cohen A, Tot T, Chiu S, Chen S, Fann J, Rosell J, Fohlin H, Smith R, Duffy S, Al E. Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades - with comments. Radiology. 2011;260(3):658–663. doi: 10.1148/radiol.11110469. - DOI - PubMed
-
- Lehman CD, Wellman RD, Buist DSM, Kerlikowske K, Tosteson ANA, Miglioretti DL, Breast Cancer Surveillance Consortium Diagnostic Accuracy of Digital Screening Mammography With and Without Computer-Aided Detection. JAMA Intern. Med. 2015;175(11):1828–1837. doi: 10.1001/jamainternmed.2015.5231. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
