

Dissecting Kawasaki disease: a state-of-the-art review
- PMID: 28656474
- PMCID: PMC5511310
- DOI: 10.1007/s00431-017-2937-5
Dissecting Kawasaki disease: a state-of-the-art review
Abstract
Kawasaki disease (KD) is a pediatric vasculitis with coronary artery aneurysms (CAA) as its main complication. The diagnosis is based on the presence of persistent fever and clinical features including exanthema, lymphadenopathy, conjunctival injection, and changes to the mucosae and extremities. Although the etiology remains unknown, the current consensus is that it is likely caused by an (infectious) trigger initiating an abnormal immune response in genetically predisposed children. Treatment consists of high dose intravenous immunoglobulin (IVIG) and is directed at preventing the development of CAA. Unfortunately, 10-20% of all patients fail to respond to IVIG and these children need additional anti-inflammatory treatment. Coronary artery lesions are diagnosed by echocardiography in the acute and subacute phases. Both absolute arterial diameters and z-scores, adjusted for height and weight, are used as criteria for CAA. Close monitoring of CAA is important as ischemic symptoms or myocardial infarction due to thrombosis or stenosis can occur. These complications are most likely to arise in the largest, so-called giant CAA. Apart from the presence of CAA, it is unclear whether KD causes an increased cardiovascular risk due to the vasculitis itself.
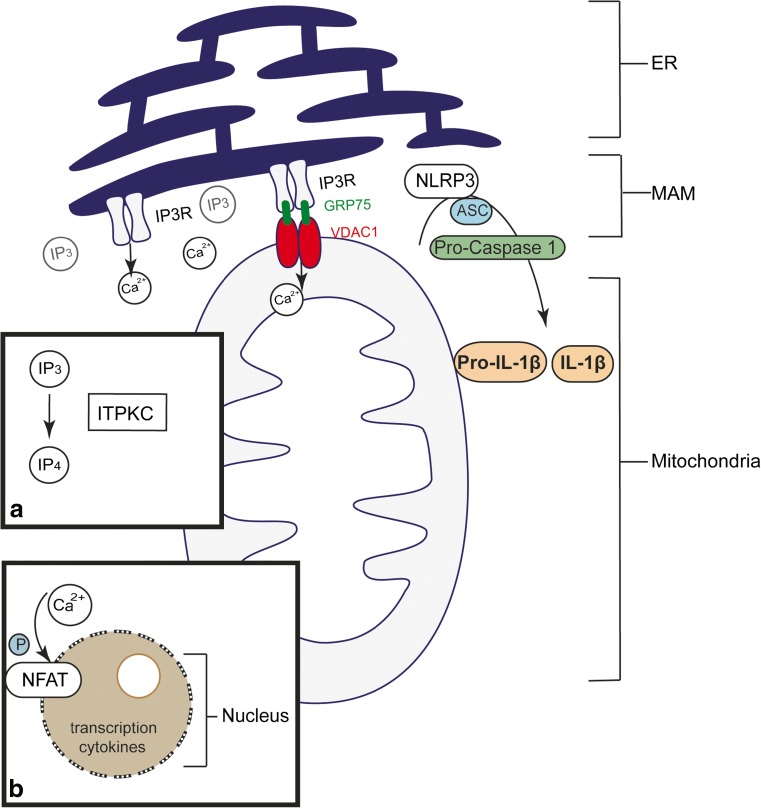
Conclusion: Many aspects of KD remain unknown, although there is growing knowledge on the etiology, treatment, and development and classification of CAA. Since children with previous KD are entering adulthood, long-term follow-up is increasingly important. What is known: • Kawasaki disease (KD) is a pediatric vasculitis with coronary artery damage as its main complication. • Although KD approaches its 50th birthday since its first description, many aspects of the disease remain poorly understood. What is new: • In recent years, multiple genetic candidate pathways involved in KD have been identified, with recently promising information about the ITPKC pathway. • As increasing numbers of KD patients are reaching adulthood, increasing information is available about the long-term consequences of coronary artery damage and broader cardiovascular risk.
Keywords: Coronary artery aneurysms; Genetics; Intravenous immunoglobulins; Kawasaki disease.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This study was supported by the Stinafo Foundation (The Hague, The Netherlands) and the Schumacher Kramer Foundation. The sponsors had no role in the study design, the data collection and analysis, the writing of the report, or the decision to submit the manuscript for publication.
Figures
Comment in
-
Kawasaki disease: what the paediatrician needs to know.Eur J Pediatr. 2017 Aug;176(8):1011. doi: 10.1007/s00431-017-2943-7. Eur J Pediatr. 2017. PMID: 28656473 No abstract available.
References
-
- Alphonse MP, Duong TT, Shumitzu C, Hoang TL, McCrindle BW, Franco A, Schurmans S, Philpott DJ, Hibberd ML, Burns J, Kuijpers TW, Yeung RS. Inositol-triphosphate 3-kinase C mediates inflammasome activation and treatment response in Kawasaki disease. J Immunol. 2016;197:3481–3489. doi: 10.4049/jimmunol.1600388. - DOI - PubMed
-
- Breunis WB, Davila S, Shimizu C, Oharaseki T, Takahashi K, van Houdt M, Khor CC, Wright VJ, Levin M, Burns JC, Burgner D, Hibberd ML, Kuijpers TW, International Kawasaki Disease Genetics C Disruption of vascular homeostasis in patients with Kawasaki disease: involvement of vascular endothelial growth factor and angiopoietins. Arthritis Rheum. 2012;64:306–315. doi: 10.1002/art.33316. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
