

Endothelial colony-forming cells and pro-angiogenic cells: clarifying definitions and their potential role in mitigating acute kidney injury
- PMID: 28656611
- PMCID: PMC5745310
- DOI: 10.1111/apha.12914
Endothelial colony-forming cells and pro-angiogenic cells: clarifying definitions and their potential role in mitigating acute kidney injury
Abstract
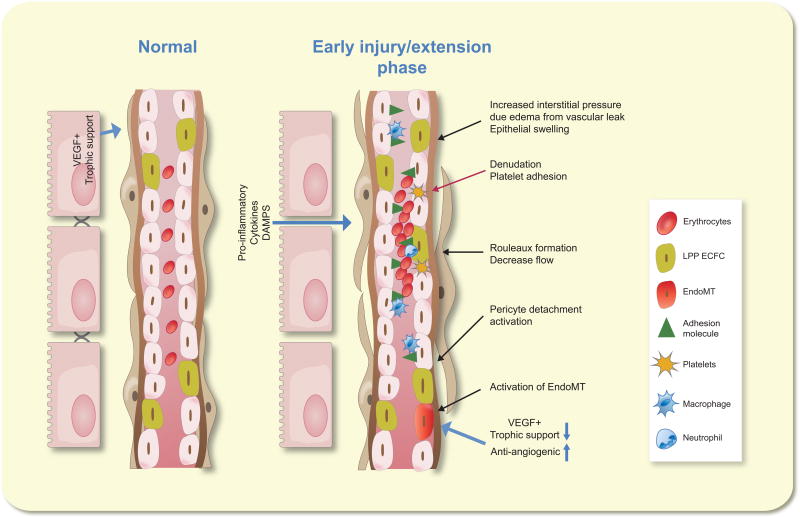
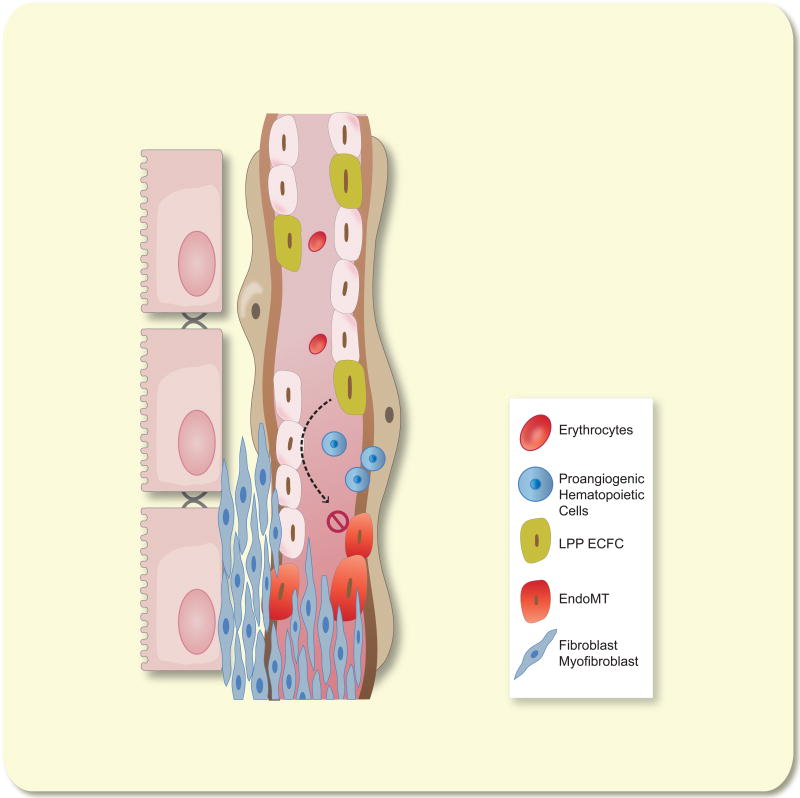
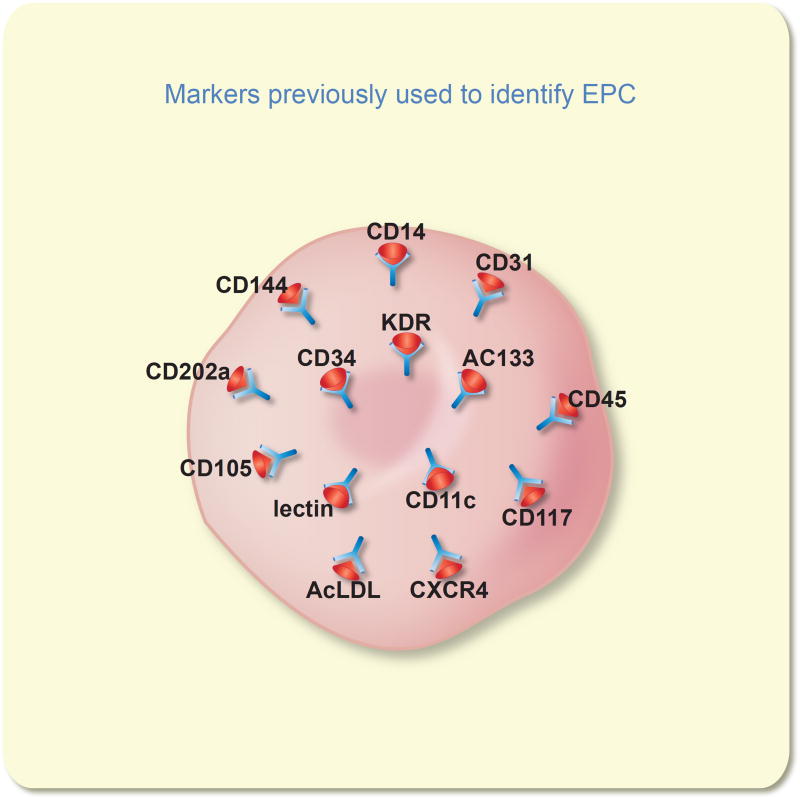
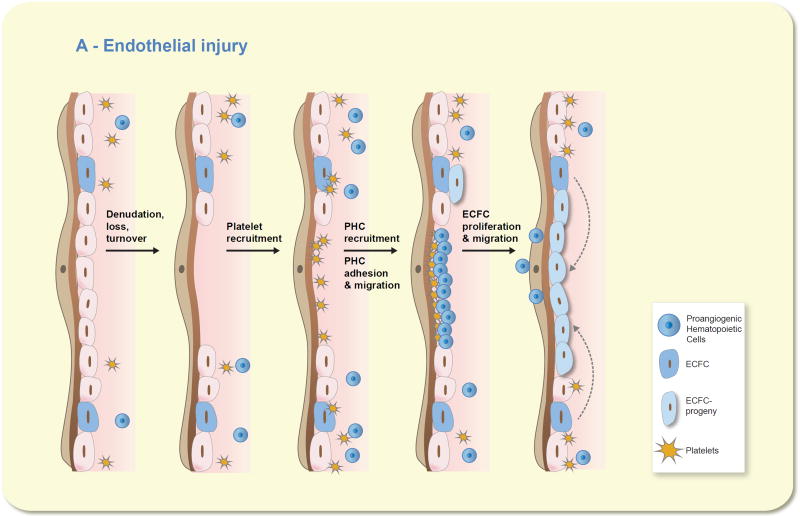
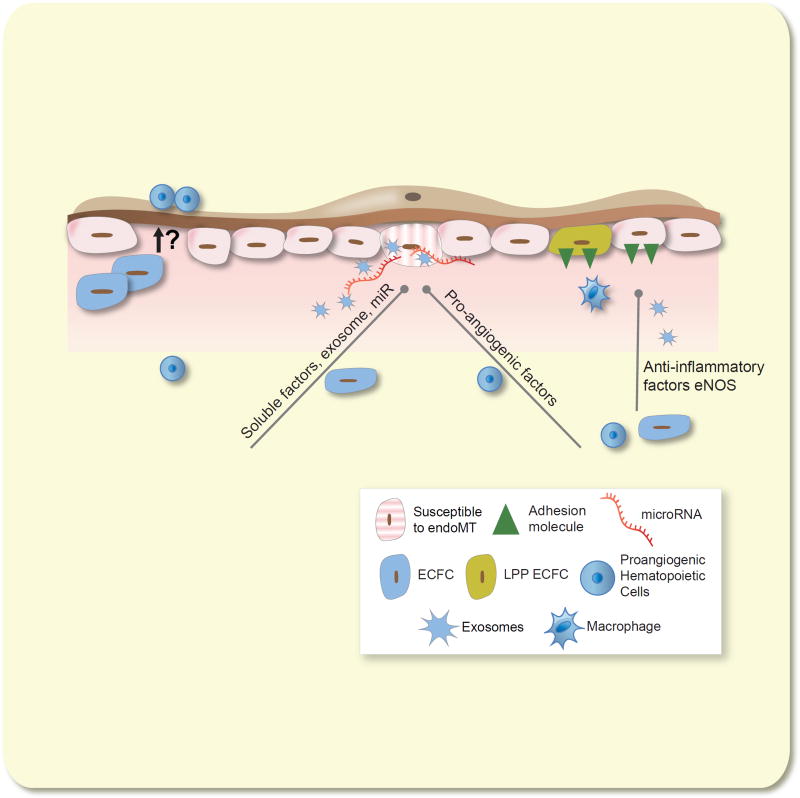
Acute kidney injury (AKI) represents a significant clinical concern that is associated with high mortality rates and also represents a significant risk factor for the development of chronic kidney disease (CKD). This article will consider alterations in renal endothelial function in the setting of AKI that may underlie impairment in renal perfusion and how inefficient vascular repair may manifest post-AKI and contribute to the potential transition to CKD. We provide updated terminology for cells previously classified as 'endothelial progenitor' that may mediate vascular repair such as pro-angiogenic cells and endothelial colony-forming cells. We consider how endothelial repair may be mediated by these different cell types following vascular injury, particularly in models of AKI. We further summarize the potential ability of these different cells to mitigate the severity of AKI, improve perfusion and maintain vascular structure in pre-clinical studies.
Keywords: angiogenesis; fibrosis; inflammation; ischaemia; rarefaction.
© 2017 Scandinavian Physiological Society. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Basile DP. The endothelial cell in ischemic acute kidney injury: implications for acute and chronic function. Kidney International. 2007;72:151–156. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
