

CD55 Deficiency, Early-Onset Protein-Losing Enteropathy, and Thrombosis
- PMID: 28657829
- PMCID: PMC6690356
- DOI: 10.1056/NEJMoa1615887
CD55 Deficiency, Early-Onset Protein-Losing Enteropathy, and Thrombosis
Abstract
Background: Studies of monogenic gastrointestinal diseases have revealed molecular pathways critical to gut homeostasis and enabled the development of targeted therapies.
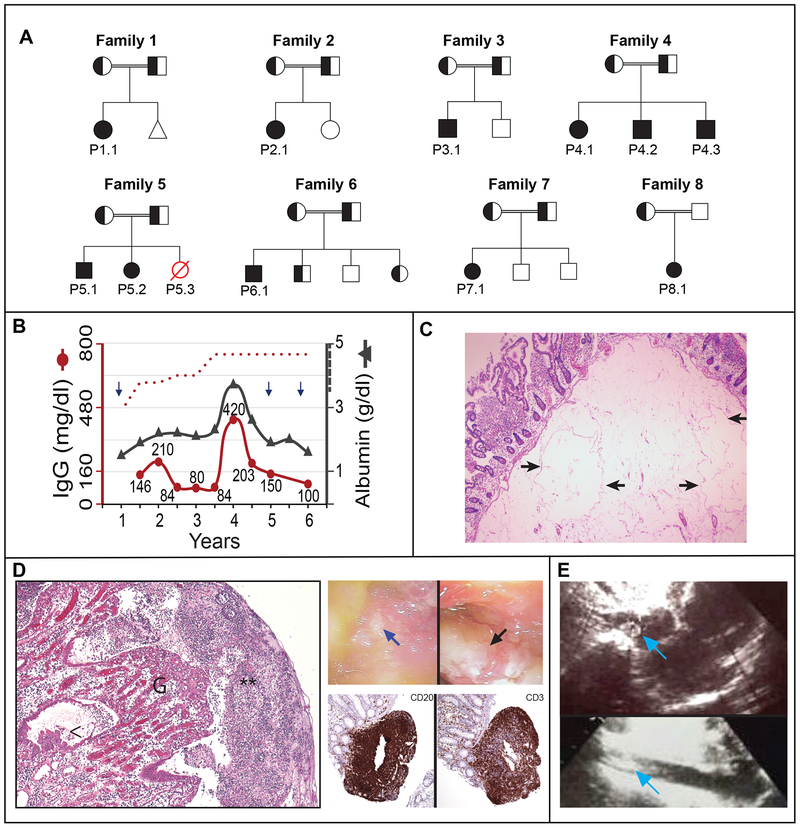
Methods: We studied 11 patients with abdominal pain and diarrhea caused by early-onset protein-losing enteropathy with primary intestinal lymphangiectasia, edema due to hypoproteinemia, malabsorption, and less frequently, bowel inflammation, recurrent infections, and angiopathic thromboembolic disease; the disorder followed an autosomal recessive pattern of inheritance. Whole-exome sequencing was performed to identify gene variants. We evaluated the function of CD55 in patients' cells, which we confirmed by means of exogenous induction of expression of CD55.
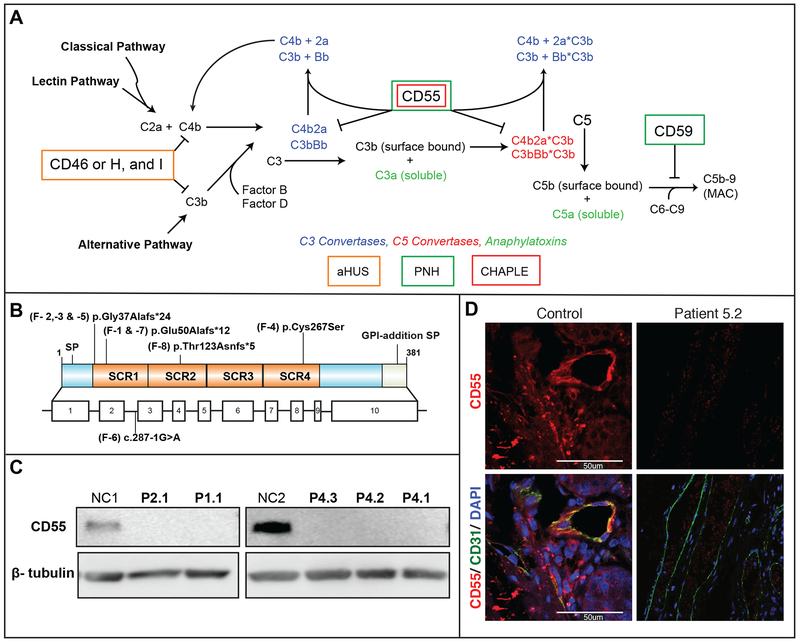
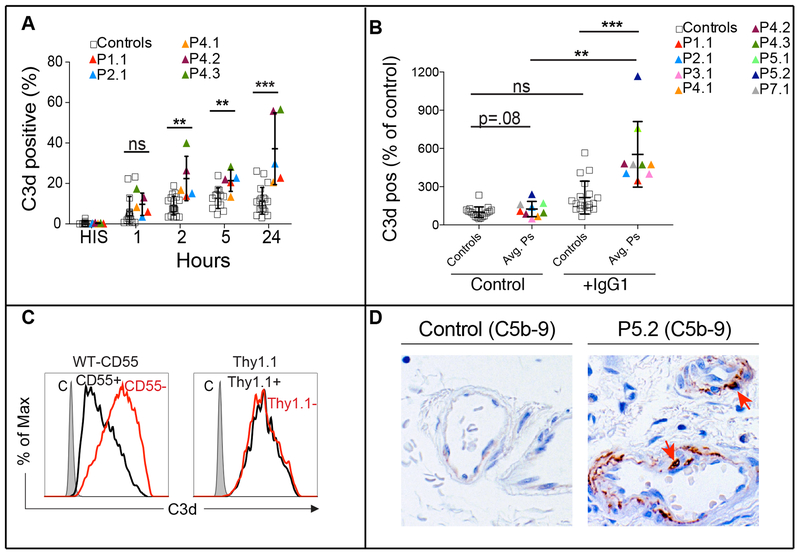
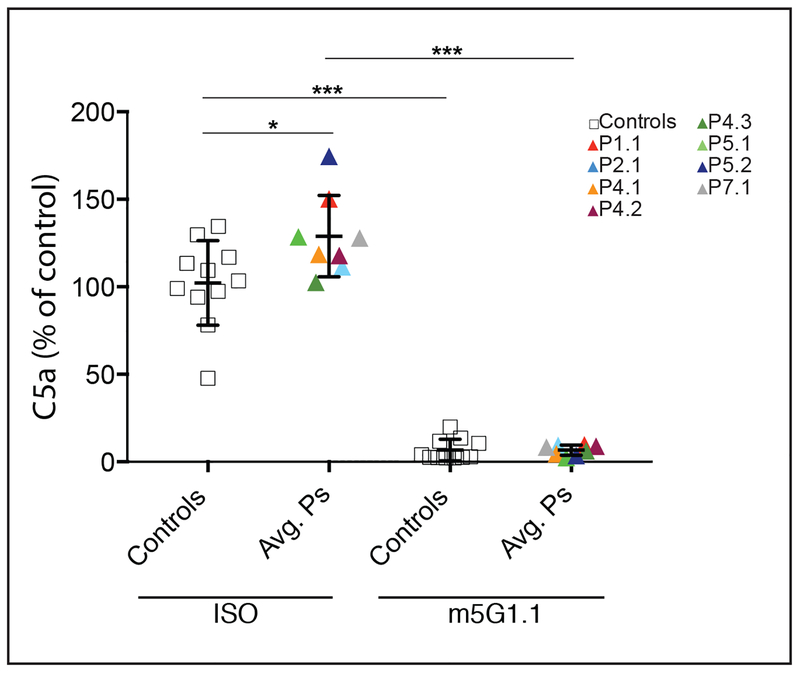
Results: We identified homozygous loss-of-function mutations in the gene encoding CD55 (decay-accelerating factor), which lead to loss of protein expression. Patients' T lymphocytes showed increased complement activation causing surface deposition of complement and the generation of soluble C5a. Costimulatory function and cytokine modulation by CD55 were defective. Genetic reconstitution of CD55 or treatment with a complement-inhibitory therapeutic antibody reversed abnormal complement activation.
Conclusions: CD55 deficiency with hyperactivation of complement, angiopathic thrombosis, and protein-losing enteropathy (the CHAPLE syndrome) is caused by abnormal complement activation due to biallelic loss-of-function mutations in CD55. (Funded by the National Institute of Allergy and Infectious Diseases and others.).
Figures
Comment in
-
CD55 Deficiency and Protein-Losing Enteropathy.N Engl J Med. 2017 Oct 12;377(15):1499. doi: 10.1056/NEJMc1710011. N Engl J Med. 2017. PMID: 29022673 No abstract available.
References
-
- Umar SB, DiBaise JK. Protein-losing enteropathy: case illustrations and clinical review. Am J Gastroenterol 2010;105:43–9; quiz 50. - PubMed
-
- Waldmann TA, Steinfeld JL, Dutcher TF, Davidson JD, Gordon RS Jr., The role of the gastrointestinal system in “idiopathic hypoproteinemia”. Gastroenterology 1961;41:197–207. - PubMed
-
- Alders M, Hogan BM, Gjini E, et al. Mutations in CCBE1 cause generalized lymph vessel dysplasia in humans. Nature genetics 2009;41:1272–4. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous