

Tumor Biology and Response to Chemotherapy Impact Breast Cancer-specific Survival in Node-positive Breast Cancer Patients Treated With Neoadjuvant Chemotherapy: Long-term Follow-up From ACOSOG Z1071 (Alliance)
- PMID: 28657941
- PMCID: PMC5755619
- DOI: 10.1097/SLA.0000000000002373
Tumor Biology and Response to Chemotherapy Impact Breast Cancer-specific Survival in Node-positive Breast Cancer Patients Treated With Neoadjuvant Chemotherapy: Long-term Follow-up From ACOSOG Z1071 (Alliance)
Abstract
Background: Women with node-positive breast cancer are at high risk for recurrence. We evaluate the impact of approximated tumor subtype and response to chemotherapy on long-term outcomes in a node-positive cohort receiving neoadjuvant chemotherapy.
Methods: ACOSOG Z1071 enrolled cT0-4N1-2 breast cancer patients treated with neoadjuvant chemotherapy from 2009 to 2011. Factors impacting breast cancer-specific survival (BCSS) and overall survival (OS) were analyzed.
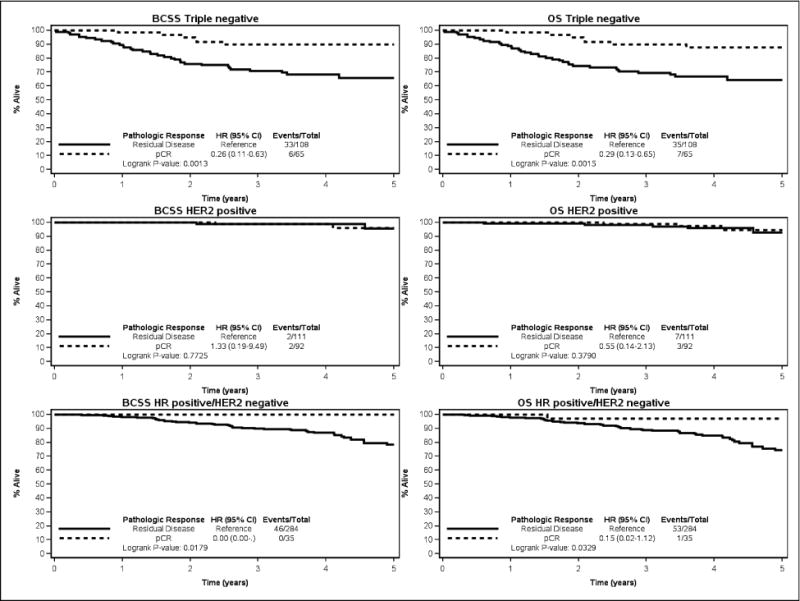
Results: Median follow-up of 701 eligible patients was 4.1 years (0.4-6.5). Ninety patients (12.8%) died from breast cancer. Approximated subtype and chemotherapy response were significantly associated with BCSS and OS (P < 0.0001). BCSS and OS were highest in patients who achieved pathologic complete response (pCR) (P < 0.0001 and P < 0.0001, respectively).Five-year BCSS was highest in human epidermal growth factor receptor 2 (HER2)-positive disease [95.8%; 95% confidence interval (CI): 87.7-98.6], followed by hormone receptor-positive/HER2-negative (80.4%; 95% CI: 73.2-85.9) and lowest in triple-negative (TNBC) (74.8%; 95% CI: 66.6-81.2; P < 0.0001). Similar patterns were seen in OS.In TNBC (n = 174), 5-year BCSS was higher in patients with pCR versus residual disease (89.8%; 95% CI: 78.8-95.3 vs 65.8%; 95% CI: 54.5-74.9; P = 0.0013). In hormone receptor-positive/HER2-negative (n = 318) disease, BCSS was 100% in patients with pCR and 78.3% (95% CI: 70.4-84.3) in those with residual disease (P = 0.018). In HER2-positive disease (n = 204) there was no difference between pCR and residual disease (96.0%; 95% CI: 83.6-99.1 vs 95.8%; 95% CI: 81.4-99.1; P = 0.77).
Conclusions: In node-positive breast cancer patients treated with neoadjuvant chemotherapy, BCSS and OS were associated with approximated subtype and chemotherapy response and were lowest in TNBC patients with residual disease. Five-year BCSS was > 95% in HER2-positive disease independent of chemotherapy response.
Trial registration: ClinicalTrials.gov NCT00881361.
Figures


References
-
- Golshan M, Cirrincione CT, Sikov WM, et al. Impact of Neoadjuvant Chemotherapy in Stage II-III Triple Negative Breast Cancer on Eligibility for Breast-Conserving Surgery and Breast Conservation Rates: Surgical Results from CALGB 40603 (Alliance) Ann Surg. 2015 Sep;262(3):434–9. discussion 438–9. - PMC - PubMed
-
- Mieog JS, van der Hage JA, van de Velde CJ. Neoadjuvant Chemotherapy for Operable Breast Cancer. Br J Surg. 2007 Oct;94(10):1189–200. - PubMed
-
- Kaufmann M, von Minckwitz G, Mamounas EP, et al. Recommendations from an International Consensus Conference on the Current Status and Future of Neoadjuvant Systemic Therapy in Primary Breast Cancer. Ann Surg Oncol. 2012 May;19(5):1508–16. - PubMed
-
- Bear HD, Anderson S, Brown A, et al. The Effect on Tumor Response of Adding Sequential Preoperative Docetaxel to Preoperative Doxorubicin and Cyclophosphamide: Preliminary Results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol. 2003 Nov 15;21(22):4165–74. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
