

Long-term Safety and Efficacy of New-Generation Drug-Eluting Stents in Women With Acute Myocardial Infarction: From the Women in Innovation and Drug-Eluting Stents (WIN-DES) Collaboration
- PMID: 28658478
- PMCID: PMC5710588
- DOI: 10.1001/jamacardio.2017.1978
Long-term Safety and Efficacy of New-Generation Drug-Eluting Stents in Women With Acute Myocardial Infarction: From the Women in Innovation and Drug-Eluting Stents (WIN-DES) Collaboration
Abstract
Importance: Women with acute myocardial infarction (MI) undergoing mechanical reperfusion remain at increased risk of adverse cardiac events and mortality compared with their male counterparts. Whether the benefits of new-generation drug-eluting stents (DES) are preserved in women with acute MI remains unclear.
Objective: To investigate the long-term safety and efficacy of new-generation DES vs early-generation DES in women with acute MI.
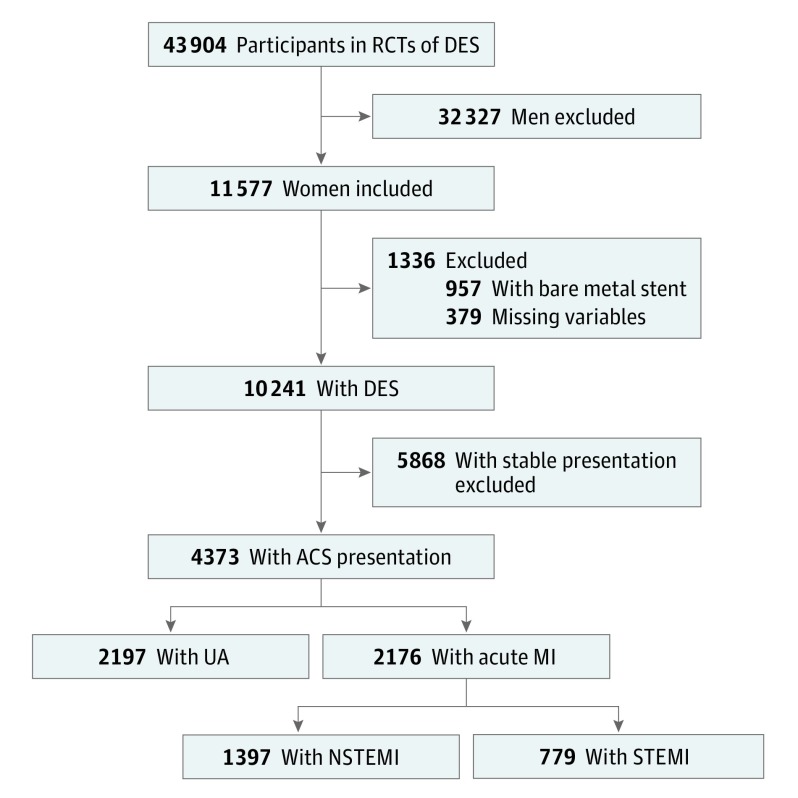
Design, setting, and participants: Collaborative, international, individual patient-level data of women enrolled in 26 randomized clinical trials of DES were analyzed between July and December 2016. Only women presenting with an acute coronary syndrome were included. Study population was categorized according to presentation with unstable angina (UA) vs acute MI. Acute MI included non-ST-segment elevation MI (NSTEMI) or ST-segment elevation MI (STEMI).
Interventions: Randomization to early- (sirolimus- or paclitaxel-eluting stents) vs new-generation (everolimus-, zotarolimus-, or biolimus-eluting stents) DES.
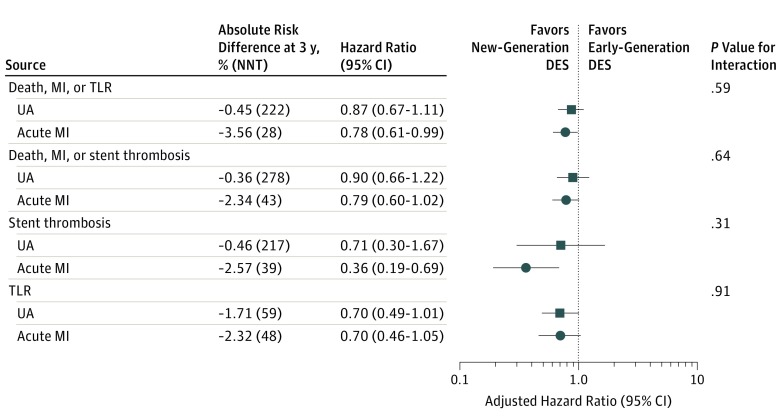
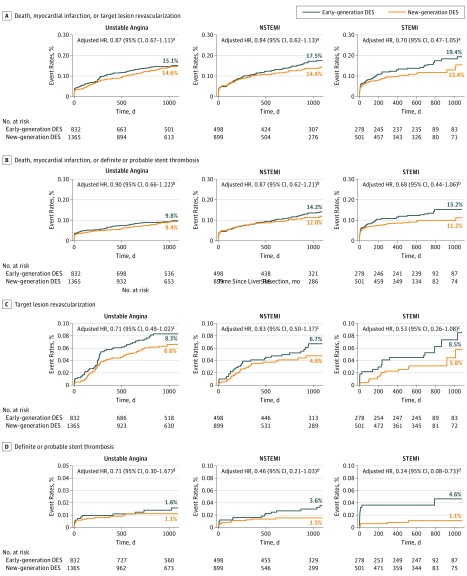
Main outcomes and measures: Composite of death, MI or target lesion revascularization, and definite or probable stent thrombosis at 3-year follow-up.
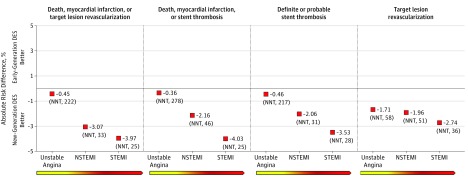
Results: Overall, the mean age of participants was 66.8 years. Of 11 577 women included in the pooled data set, 4373 (37.8%) had an acute coronary syndrome as clinical presentation. Of these 4373 women, 2176 (49.8%) presented with an acute MI. In women with acute MI, new-generation DES were associated with lower risk of death, MI or target lesion revascularization (14.9% vs 18.4%; absolute risk difference, -3.5%; number needed to treat [NNT], 29; adjusted hazard ratio, 0.78; 95% CI, 0.61-0.99), and definite or probable stent thrombosis (1.4% vs 4.0%; absolute risk difference, -2.6%; NNT, 46; adjusted hazard ratio, 0.36; 95% CI, 0.19-0.69) without evidence of interaction for both end points compared with women without acute MI (P for interaction = .59 and P for interaction = .31, respectively). A graded absolute benefit with use of new-generation DES was observed in the transition from UA, to NSTEMI, and to STEMI (for death, MI, or target lesion revascularization: UA, -0.5% [NNT, 222]; NSTEMI, -3.1% [NNT, 33]; STEMI, -4.0% [NNT, 25] and for definite or probable ST: UA, -0.4% [NNT, 278]; NSTEMI, -2.2% [NNT, 46]; STEMI, -4.0% [NNT, 25]).
Conclusions and relevance: New-generation DES are associated with consistent and durable benefits over 3 years in women presenting with acute MI. The magnitude of these benefits appeared to be greater per increase in severity of acute coronary syndrome.
Conflict of interest statement
Figures
References
-
- Pancholy SB, Shantha GP, Patel T, Cheskin LJ. Sex differences in short-term and long-term all-cause mortality among patients with ST-segment elevation myocardial infarction treated by primary percutaneous intervention: a meta-analysis. JAMA Intern Med. 2014;174(11):1822-1830. - PubMed
-
- Benamer H, Tafflet M, Bataille S, et al. ; CARDIO-ARHIF Registry Investigators . Female gender is an independent predictor of in-hospital mortality after STEMI in the era of primary PCI: insights from the greater Paris area PCI Registry. EuroIntervention. 2011;6(9):1073-1079. - PubMed
-
- Yu J, Mehran R, Grinfeld L, et al. . Sex-based differences in bleeding and long term adverse events after percutaneous coronary intervention for acute myocardial infarction: three year results from the HORIZONS-AMI trial. Catheter Cardiovasc Interv. 2015;85(3):359-368. - PubMed
-
- Jackson EA, Moscucci M, Smith DE, et al. . The association of sex with outcomes among patients undergoing primary percutaneous coronary intervention for ST elevation myocardial infarction in the contemporary era: insights from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2). Am Heart J. 2011;161(1):106-112.e1. - PubMed
-
- Wijnbergen I, Tijssen J, van ’t Veer M, Michels R, Pijls NH. Gender differences in long-term outcome after primary percutaneous intervention for ST-segment elevation myocardial infarction. Catheter Cardiovasc Interv. 2013;82(3):379-384. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
