

Childhood intelligence in relation to major causes of death in 68 year follow-up: prospective population study
- PMID: 28659274
- PMCID: PMC5485432
- DOI: 10.1136/bmj.j2708
Childhood intelligence in relation to major causes of death in 68 year follow-up: prospective population study
Abstract
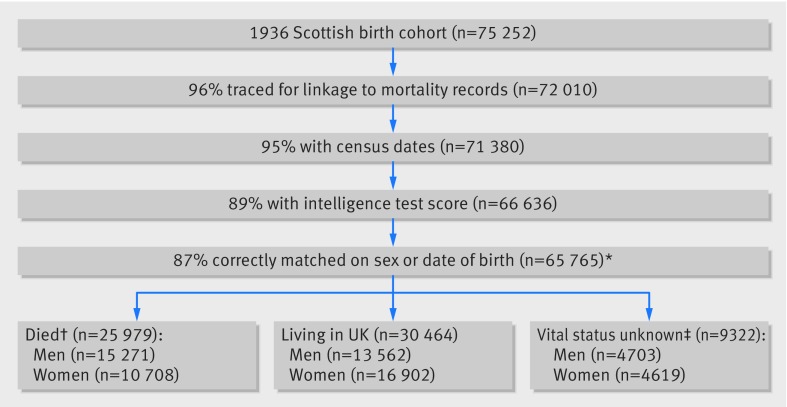
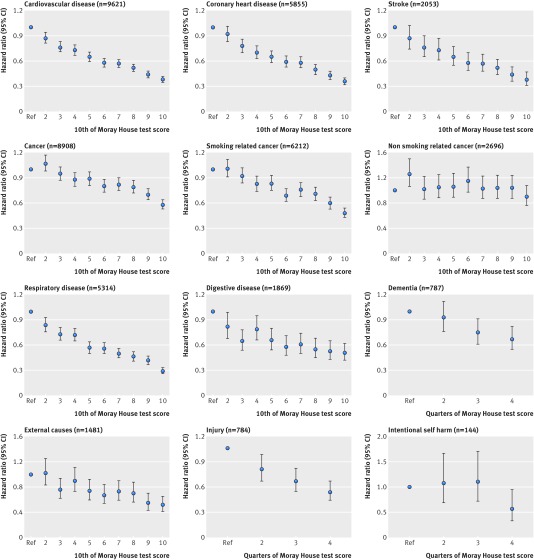
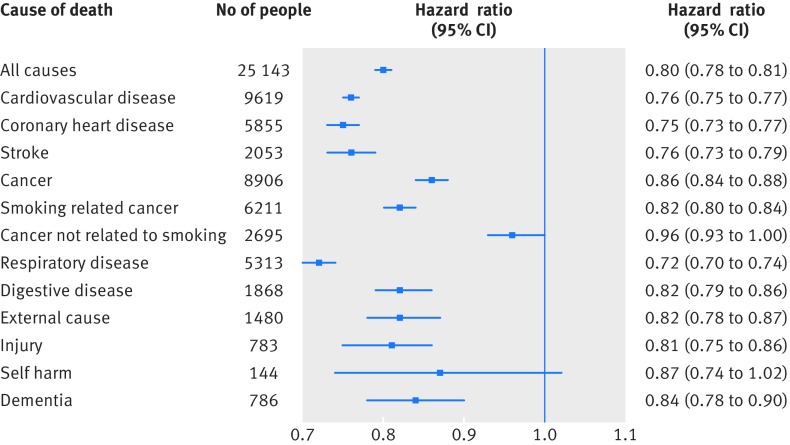
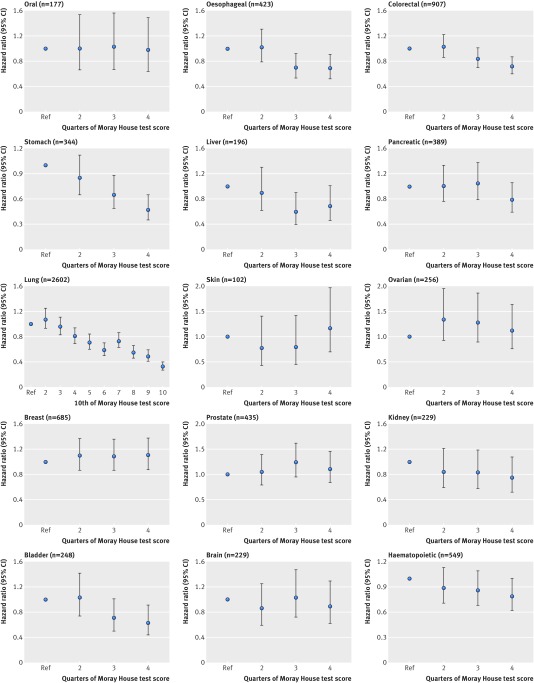
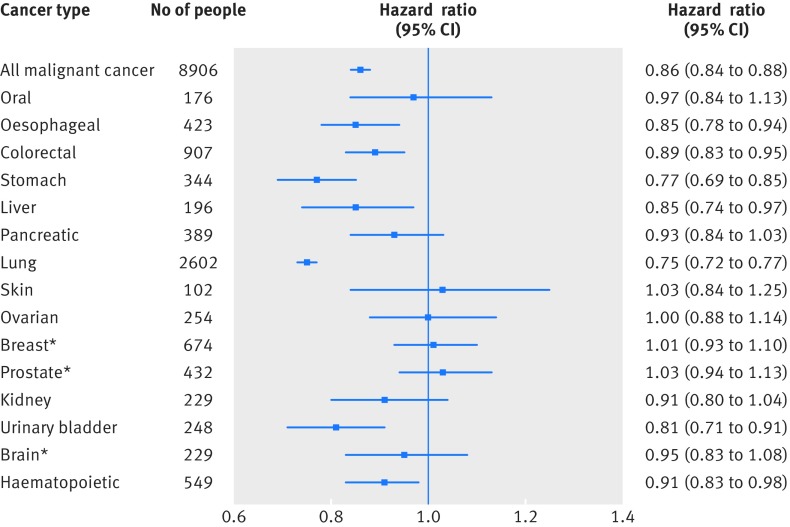
Objectives To examine the association between intelligence measured in childhood and leading causes of death in men and women over the life course.Design Prospective cohort study based on a whole population of participants born in Scotland in 1936 and linked to mortality data across 68 years of follow-up.Setting Scotland.Participants 33 536 men and 32 229 women who were participants in the Scottish Mental Survey of 1947 (SMS1947) and who could be linked to cause of death data up to December 2015.Main outcome measures Cause specific mortality, including from coronary heart disease, stroke, specific cancer types, respiratory disease, digestive disease, external causes, and dementia.Results Childhood intelligence was inversely associated with all major causes of death. The age and sex adjusted hazard ratios (and 95% confidence intervals) per 1 SD (about 15 points) advantage in intelligence test score were strongest for respiratory disease (0.72, 0.70 to 0.74), coronary heart disease (0.75, 0.73 to 0.77), and stroke (0.76, 0.73 to 0.79). Other notable associations (all P<0.001) were observed for deaths from injury (0.81, 0.75 to 0.86), smoking related cancers (0.82, 0.80 to 0.84), digestive disease (0.82, 0.79 to 0.86), and dementia (0.84, 0.78 to 0.90). Weak associations were apparent for suicide (0.87, 0.74 to 1.02) and deaths from cancer not related to smoking (0.96, 0.93 to 1.00), and their confidence intervals included unity. There was a suggestion that childhood intelligence was somewhat more strongly related to coronary heart disease, smoking related cancers, respiratory disease, and dementia in women than men (P value for interactions <0.001, 0.02, <0.001, and 0.02, respectively).Childhood intelligence was related to selected cancer presentations, including lung (0.75, 0.72 to 0.77), stomach (0.77, 0.69 to 0.85), bladder (0.81, 0.71 to 0.91), oesophageal (0.85, 0.78 to 0.94), liver (0.85, 0.74 to 0.97), colorectal (0.89, 0.83 to 0.95), and haematopoietic (0.91, 0.83 to 0.98). Sensitivity analyses on a representative subsample of the cohort observed only small attenuation of the estimated effect of intelligence (by 10-26%) after adjustment for potential confounders, including three indicators of childhood socioeconomic status. In a replication sample from Scotland, in a similar birth year cohort and follow-up period, smoking and adult socioeconomic status partially attenuated (by 16-58%) the association of intelligence with outcome rates.Conclusions In a whole national population year of birth cohort followed over the life course from age 11 to age 79, higher scores on a well validated childhood intelligence test were associated with lower risk of mortality ascribed to coronary heart disease and stroke, cancers related to smoking (particularly lung and stomach), respiratory diseases, digestive diseases, injury, and dementia.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: that IJD was the recipient of an MRC grant for staff and consumables to complete the work, from which salaries were paid for CMC, CEB, and IC; no other financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Higher IQ in childhood is linked to a longer life.BMJ. 2017 Jun 28;357:j2932. doi: 10.1136/bmj.j2932. BMJ. 2017. PMID: 28659266 Free PMC article.
-
Healthcare for the many.BMJ. 2017 Jun 29;357:j3122. doi: 10.1136/bmj.j3122. BMJ. 2017. PMID: 28663168 No abstract available.
References
-
- Calvin CM, Deary IJ, Fenton C, et al. Intelligence in youth and all-cause-mortality: systematic review with meta-analysis. Int J Epidemiol 2011;40:626-44. 10.1093/ije/dyq190 pmid:21037248. - DOI - PMC - PubMed
-
- Batty GD, Wennerstad KM, Smith GD, et al. IQ in early adulthood and mortality by middle age: cohort study of 1 million Swedish men. Epidemiology 2009;20:100-9. 10.1097/EDE.0b013e31818ba076 pmid:19234402. - DOI - PubMed
-
- Lawlor DA, Batty GD, Clark H, McIntyre S, Leon DA. Association of childhood intelligence with risk of coronary heart disease and stroke: findings from the Aberdeen Children of the 1950s cohort study. Eur J Epidemiol 2008;23:695-706. 10.1007/s10654-008-9281-z pmid:18704700. - DOI - PubMed
-
- Leon DA, Lawlor DA, Clark H, Batty GD, Macintyre S. The association of childhood intelligence with mortality risk from adolescence to middle age: Findings from the Aberdeen Children of the 1950s cohort study. Intelligence 2009;37:520-8 10.1016/j.intell.2008.11.004. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources