

Effects of Assist-As-Needed Upper Extremity Robotic Therapy after Incomplete Spinal Cord Injury: A Parallel-Group Controlled Trial
- PMID: 28659784
- PMCID: PMC5469353
- DOI: 10.3389/fnbot.2017.00026
Effects of Assist-As-Needed Upper Extremity Robotic Therapy after Incomplete Spinal Cord Injury: A Parallel-Group Controlled Trial
Abstract
Background: Robotic rehabilitation of the upper limb following neurological injury has been supported through several large clinical studies for individuals with chronic stroke. The application of robotic rehabilitation to the treatment of other neurological injuries is less developed, despite indications that strategies successful for restoration of motor capability following stroke may benefit individuals with incomplete spinal cord injury (SCI) as well. Although recent studies suggest that robot-aided rehabilitation might be beneficial after incomplete SCI, it is still unclear what type of robot-aided intervention contributes to motor recovery.
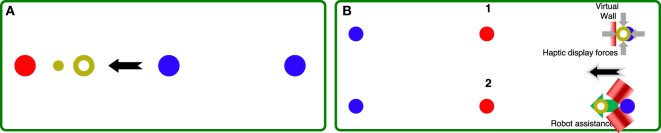
Methods: We developed a novel assist-as-needed (AAN) robotic controller to adjust challenge and robotic assistance continuously during rehabilitation therapy delivered via an upper extremity exoskeleton, the MAHI Exo-II, to train independent elbow and wrist joint movements. We further enrolled seventeen patients with incomplete spinal cord injury (AIS C and D levels) in a parallel-group balanced controlled trial to test the efficacy of the AAN controller, compared to a subject-triggered (ST) controller that does not adjust assistance or challenge levels continuously during therapy. The conducted study is a stage two, development-of-concept pilot study.
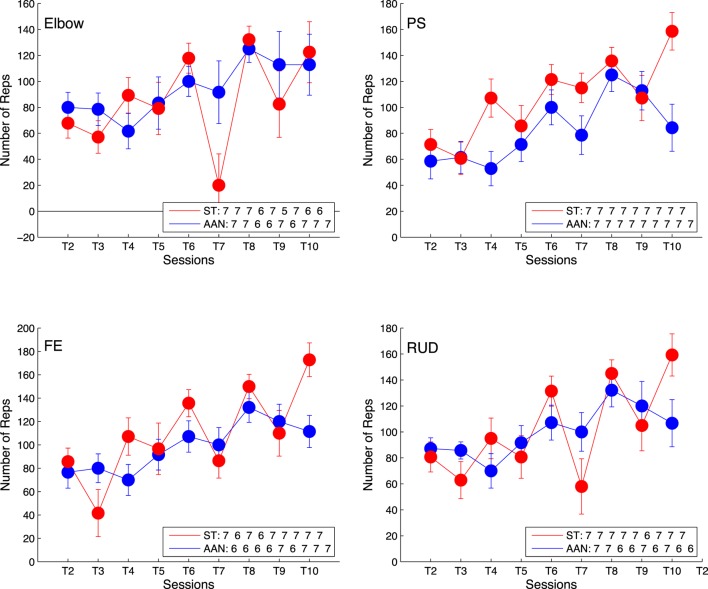
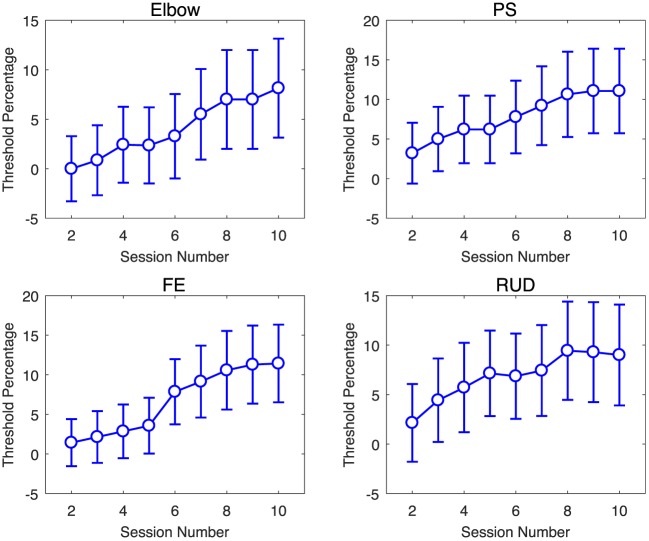
Results: We validated the AAN controller in its capability of modulating assistance and challenge during therapy via analysis of longitudinal robotic metrics. For the selected primary outcome measure, the pre-post difference in ARAT score, no statistically significant change was measured in either group of subjects. Ancillary analysis of secondary outcome measures obtained via robotic testing indicates gradual improvement in movement quality during the therapy program in both groups, with the AAN controller affording greater increases in movement quality over the ST controller.
Conclusion: The present study demonstrates feasibility of subject-adaptive robotic therapy after incomplete spinal cord injury, but does not demonstrate gains in arm function occurring as a result of the robot-assisted rehabilitation program, nor differential gains obtained as a result of the developed AAN controller. Further research is warranted to better quantify the recovery potential provided by AAN control strategies for robotic rehabilitation of the upper limb following incomplete SCI. ClinicalTrials.gov registration number: NCT02803255.
Keywords: adaptive control; assist-as-needed therapy; incomplete spinal cord injury; motor learning; robot-aided rehabilitation.
Figures






References
-
- Cai L. L., Fong A. J., Otoshi C. K., Liang Y., Burdick J. W., Roy R. R., et al. (2006). Implications of assist-as-needed robotic step training after a complete spinal cord injury on intrinsic strategies of motor learning. J. Neurosci. 26, 10564–10568. 10.1523/JNEUROSCI.2266-06.2006 - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials