

Change in Use of Sleep Medications After Gastric Bypass Surgery or Intensive Lifestyle Treatment in Adults with Obesity
- PMID: 28660652
- PMCID: PMC5533175
- DOI: 10.1002/oby.21908
Change in Use of Sleep Medications After Gastric Bypass Surgery or Intensive Lifestyle Treatment in Adults with Obesity
Abstract
Objective: To examine the change in use of hypnotics and/or sedatives after gastric bypass surgery or intensive lifestyle modification in adults with obesity.
Methods: Adults with obesity who underwent gastric bypass surgery or initiated intensive lifestyle modification between 2007 and 2012 were identified through the Scandinavian Obesity Surgery Registry and a Swedish commercial weight loss database. The two cohorts were matched on BMI, age, sex, education, history of hypnotics and/or sedatives use, and treatment year (surgery n = 20,626; lifestyle n = 11,973; 77% women, mean age 41 years, mean BMI 41 kg/m2 ). The proportion of participants with filled hypnotics and/or sedatives prescriptions was compared yearly for 3 years.
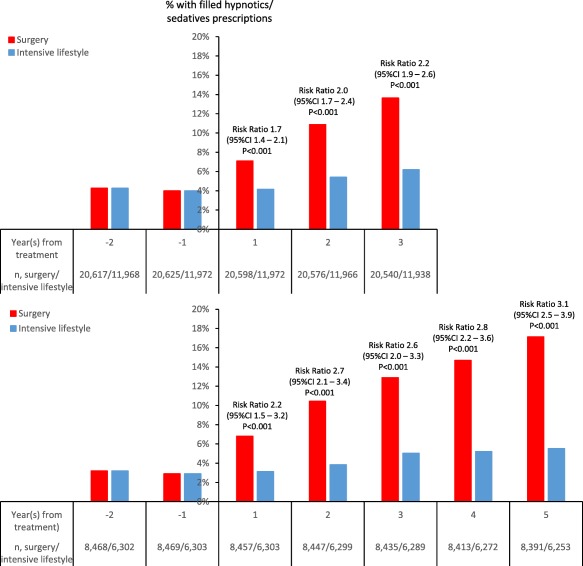
Results: In the matched treatment cohorts, 4% had filled prescriptions for hypnotics and/or sedatives during the year before treatment. At 1 year follow-up, following an average weight loss of 37 kg and 18 kg in the surgery and intensive lifestyle cohorts, respectively, this proportion had increased to 7% in the surgery cohort but remained at 4% in the intensive lifestyle cohort (risk ratio 1.7; 95% CI: 1.4-2.1); at 2 years, the proportion had increased to 11% versus 5% (risk ratio 2.0; 95% CI: 1.7-2.4); and at 3 years, it had increased to 14% versus 6% (risk ratio 2.2; 95% CI: 1.9-2.6).
Conclusions: Gastric bypass surgery was associated with increased use of hypnotics and/or sedatives compared with intensive lifestyle modification.
© 2017 The Authors. Obesity published by Wiley Periodicals, Inc. on behalf of The Obesity Society (TOS).
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
