

Major haemorrhage requiring transarterial embolisation following open biopsy of an unusual neck mass
- PMID: 28660821
- PMCID: PMC5697019
- DOI: 10.1308/rcsann.2017.0073
Major haemorrhage requiring transarterial embolisation following open biopsy of an unusual neck mass
Abstract
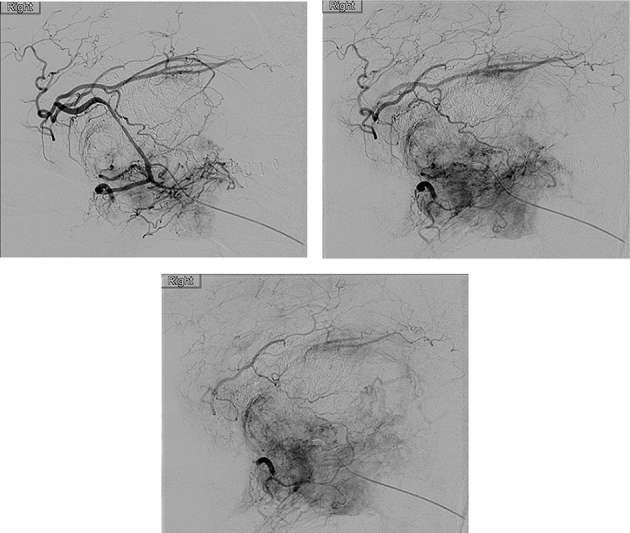
A 65-year-old man presented with a right supraclavicular neck mass and right arm pain. Magnetic resonance imaging revealed a 96mm lesion in the upper thoracic paraspinal region extending into the deep supraclavicular fossa. The presentation was consistent with a sarcoma or lymphoma but fine needle aspiration was inconclusive. During open biopsy of the lesion, the patient had a rapid intraoperative haemorrhage of 1l from the tumour. Haemostasis could only be achieved by transarterial embolisation of the feeding vessel and the biopsy result confirmed Ewing's sarcoma. Open biopsy is considered the gold standard in the diagnosis of certain tumour types; however, the morbidity from haemorrhage must be considered. This case highlights the key role that transarterial embolisation can play in achieving haemostasis in the neck.
Keywords: Embolisation; Ewing’s; Haemorrhage; Neck mass; Sarcoma.
Figures



References
-
- Ellison E, LaPuerta P, Martin SE. Supraclavicular masses: results of a series of 309 cases biopsied by fine needle aspiration. Head Neck 1999; : 239–246. - PubMed
-
- Lefebvre JL, Coche-Dequeant B, Van JT et al. . Cervical lymph nodes from an unknown primary tumor in 190 patients. Am J Surg 1990; : 443–446. - PubMed
-
- Eichenauer DA, Engert A, André M et al. . Hodgkin’s lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2014; 25(Suppl 3): iii70–iii75. - PubMed
-
- ESMO/European Sarcoma Network Working Group. Soft tissue and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2014; 25(Suppl 3): iii102–iii112. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical