

Autoantibodies in juvenile-onset myositis: Their diagnostic value and associated clinical phenotype in a large UK cohort
- PMID: 28663002
- PMCID: PMC5656106
- DOI: 10.1016/j.jaut.2017.06.007
Autoantibodies in juvenile-onset myositis: Their diagnostic value and associated clinical phenotype in a large UK cohort
Abstract
Objectives: Juvenile myositis is a rare and heterogeneous disease. Diagnosis is often difficult but early treatment is important in reducing the risk of associated morbidity and poor outcomes. Myositis specific autoantibodies have been described in both juvenile and adult patients with myositis and can be helpful in dividing patients into clinically homogenous groups. We aimed to explore the utility of myositis specific autoantibodies as diagnostic and prognostic biomarkers in patients with juvenile-onset disease.
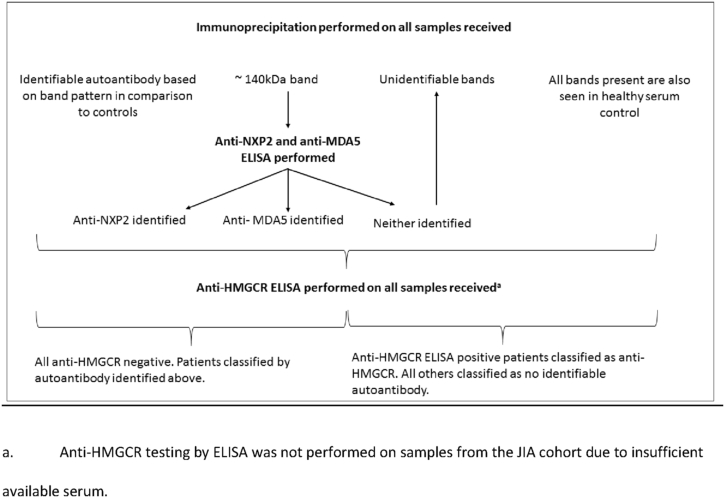
Methods: Using radio-labelled immunoprecipitation and previously validated ELISAs we examined the presence of myositis specific autoantibodies in 380 patients with juvenile-onset myositis in addition to, 318 patients with juvenile idiopathic arthritis, 21 patients with juvenile-onset SLE, 27 patients with muscular dystrophies, and 48 healthy children.
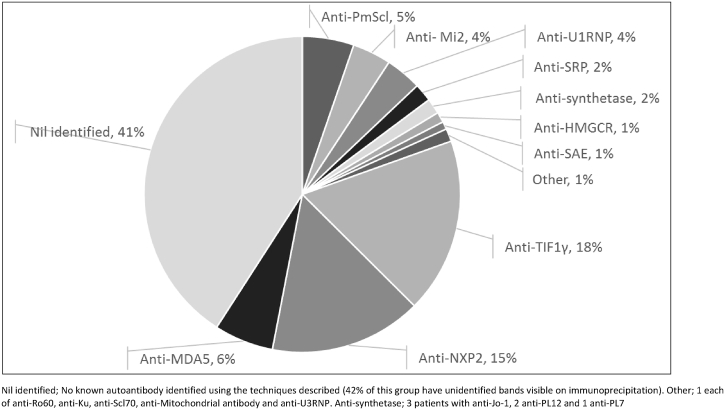
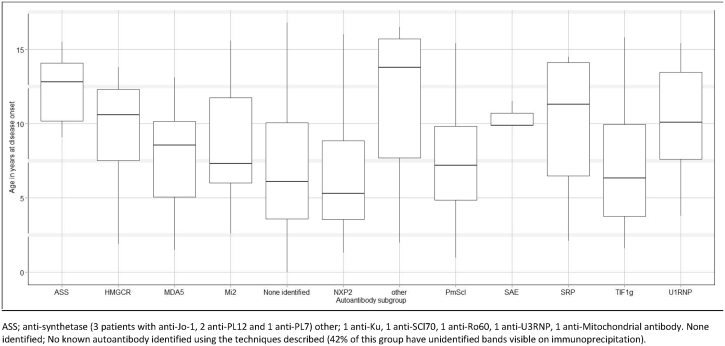
Results: An autoantibody was identified in 60% of juvenile-onset myositis patients. Myositis specific autoantibodies (49% patients) were exclusively found in patients with myositis and with the exception of one case were mutually exclusive and not found in conjunction with another autoantibody. Autoantibody subtypes were associated with age at disease onset, key clinical disease features and treatment received.
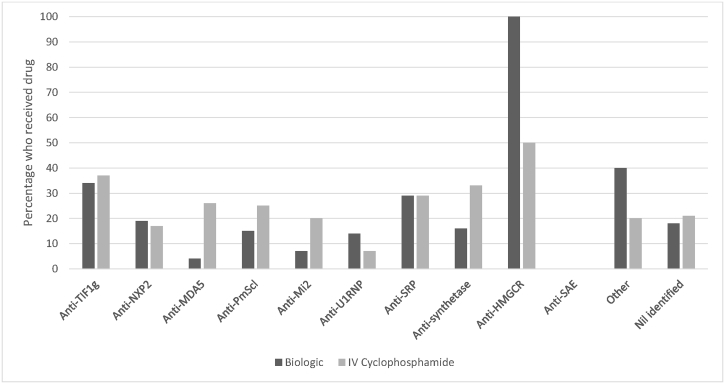
Conclusions: In juvenile patients the identification of a myositis specific autoantibody is highly suggestive of myositis. Autoantibodies can be identified in the majority of affected children and provide useful prognostic information. There is evidence of a differential treatment approach and patients with anti-TIF1γ autoantibodies are significantly more likely to receive aggressive treatment with IV cyclophosphamide and/or biologic drugs, clear trends are also visible in other autoantibody subgroups.
Keywords: Autoantibody; Autoimmune disease; Myopathy; Myositis; Paediatric rheumatology; Phenotype.
Copyright © 2017 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Martin N., Krol P., Smith S., Murray K., Pilkington C.A., Davidson J.E. A national registry for juvenile dermatomyositis and other paediatric idiopathic inflammatory myopathies: 10 years' experience; the Juvenile Dermatomyositis National (UK and Ireland) Cohort Biomarker Study and Repository for Idiopathic Inflammatory Myopathies. Rheumatology. 2011;50(1):137–145. - PMC - PubMed
-
- Gunawardena H., Wedderburn L.R., North J., Betteridge Z., Dunphy J., Chinoy H. Clinical associations of autoantibodies to a p155/140 kDa doublet protein in juvenile dermatomyositis. Rheumatology. 2008;47(3):324–328. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
