

Increased Curvature of the Tentorium Cerebelli in Idiopathic Intracranial Hypertension
- PMID: 28663268
- PMCID: PMC7963697
- DOI: 10.3174/ajnr.A5289
Increased Curvature of the Tentorium Cerebelli in Idiopathic Intracranial Hypertension
Abstract
Background and purpose: Transverse sinus effacement is detectable on MRV examinations in almost all patients with idiopathic intracranial hypertension. This effacement of the transverse sinus is presumed to be mediated by elevation of intracranial pressure, resulting in compression and inward collapse of the dural margins of the sinus. We sought to establish whether supratentorial broad-based downward deformity of the tentorium might explain transverse sinus effacement in idiopathic intracranial hypertension.
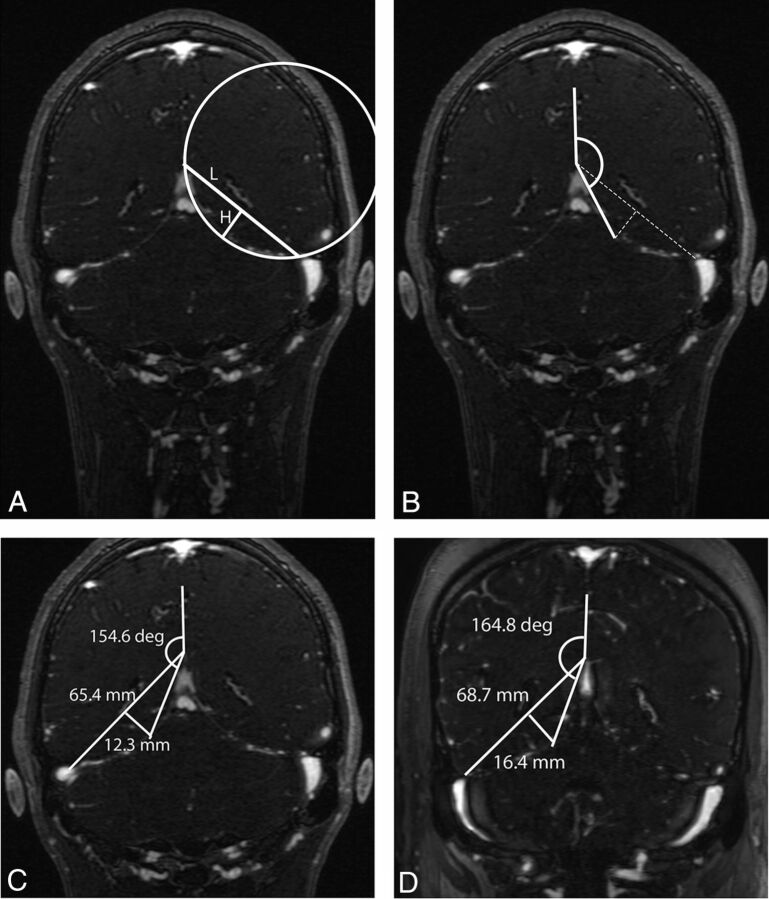
Materials and methods: MRV examinations of 53 adult patients with idiopathic intracranial hypertension were reviewed retrospectively and compared with 58 contemporaneously acquired controls. The curvature of the tentorium with reference to a line connecting the transverse sinus laterally with the confluence of the tentorial leaves medially was calculated as a segment of a circle. The height and area of the segment and the angle subtended by the midpoint of the tentorium from the falx were calculated.
Results: The height and area of the segment described by the chord connecting the transverse sinus with the apex of the tentorial confluence and subtended midtentorial angle were greater in the idiopathic intracranial hypertension group; this finding supports the hypothesis that increased tentorial bowing is present in idiopathic intracranial hypertension.
Conclusions: Increased bowing of the tentorium in patients with idiopathic intracranial hypertension compared with controls is a new observation, lending itself to new hypotheses on the nature and localization of elevated intracranial pressure in idiopathic intracranial hypertension. Bowing of the tentorium may play a part in distorting the contour of the transverse sinuses, resulting, at least in part, in the effacement of the transverse sinuses in idiopathic intracranial hypertension.
© 2017 by American Journal of Neuroradiology.
Figures
Similar articles
-
Transverse Sinus Stenosis Is the Most Sensitive MR Imaging Correlate of Idiopathic Intracranial Hypertension.AJNR Am J Neuroradiol. 2017 Mar;38(3):471-477. doi: 10.3174/ajnr.A5055. Epub 2017 Jan 19. AJNR Am J Neuroradiol. 2017. PMID: 28104635 Free PMC article.
-
Visualization of the tentorial innervation of human dura mater.J Anat. 2017 Nov;231(5):683-689. doi: 10.1111/joa.12659. Epub 2017 Jul 10. J Anat. 2017. PMID: 28695607 Free PMC article.
-
Sigmoid Sinus Diverticulum, Dehiscence, and Venous Sinus Stenosis: Potential Causes of Pulsatile Tinnitus in Patients with Idiopathic Intracranial Hypertension?AJNR Am J Neuroradiol. 2017 Sep;38(9):1783-1788. doi: 10.3174/ajnr.A5277. Epub 2017 Jul 13. AJNR Am J Neuroradiol. 2017. PMID: 28705815 Free PMC article.
-
Starling resistors, autoregulation of cerebral perfusion and the pathogenesis of idiopathic intracranial hypertension.Panminerva Med. 2017 Mar;59(1):76-89. doi: 10.23736/S0031-0808.16.03248-1. Epub 2016 Sep 6. Panminerva Med. 2017. PMID: 27598891 Review.
-
Dural sinus collapsibility, idiopathic intracranial hypertension, and the pathogenesis of chronic migraine.Neurol Sci. 2019 May;40(Suppl 1):59-70. doi: 10.1007/s10072-019-03775-w. Neurol Sci. 2019. PMID: 30838545 Review.
Cited by
-
A retrospective anatomical study of the cerebral dural venous sinus outflow pathways utilizing three-dimensional rotational venography.Brain Circ. 2022 Mar 21;8(1):38-44. doi: 10.4103/bc.bc_76_21. eCollection 2022 Jan-Mar. Brain Circ. 2022. PMID: 35372723 Free PMC article.
-
The Occipital Emissary Vein: A Possible Marker for Pseudotumor Cerebri.AJNR Am J Neuroradiol. 2019 Jun;40(6):973-978. doi: 10.3174/ajnr.A6061. Epub 2019 May 9. AJNR Am J Neuroradiol. 2019. PMID: 31072972 Free PMC article.
-
Contrast-Enhanced 3D-FLAIR Imaging of the Optic Nerve and Optic Nerve Head: Novel Neuroimaging Findings of Idiopathic Intracranial Hypertension.AJNR Am J Neuroradiol. 2019 Feb;40(2):334-339. doi: 10.3174/ajnr.A5937. Epub 2019 Jan 24. AJNR Am J Neuroradiol. 2019. PMID: 30679213 Free PMC article.
-
Tentorium Cerebelli: Muscles, Ligaments, and Dura Mater, Part 1.Cureus. 2019 Sep 9;11(9):e5601. doi: 10.7759/cureus.5601. Cureus. 2019. PMID: 31700714 Free PMC article. Review.
-
Reduced Jet Velocity in Venous Flow after CSF Drainage: Assessing Hemodynamic Causes of Pulsatile Tinnitus.AJNR Am J Neuroradiol. 2019 May;40(5):849-854. doi: 10.3174/ajnr.A6043. Epub 2019 Apr 25. AJNR Am J Neuroradiol. 2019. PMID: 31023664 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous