

Appendiceal Mucinous Neoplasms: Diagnosis and Management
- PMID: 28663356
- PMCID: PMC5599200
- DOI: 10.1634/theoncologist.2017-0081
Appendiceal Mucinous Neoplasms: Diagnosis and Management
Erratum in
-
Appendiceal Mucinous Neoplasms: Diagnosis and Management.Oncologist. 2018 Jan;23(1):137. doi: 10.1634/theoncologist.2017-0081erratum. Oncologist. 2018. PMID: 29317549 Free PMC article. No abstract available.
Abstract
Objective: Appendiceal mucinous neoplasms (AMNs) are a rare and heterogeneous disease for which clinical management is challenging. We aim to review the literature regarding modalities of treatment to guide the management of AMNs.
Methods and review criteria: We conducted a PubMed search in February 2016 for English-language publications, using the terms "appendiceal," "appendix," "carcinoma," "cancer," "mucinous," "treatment," "genes," "target," "genomic," and terms listed in the articles' subheadings. Published reports and abstracts from the American Society of Clinical Oncology meetings were also searched.
Results: In this review, we summarize current data and controversies in AMN classification, clinical presentation, molecular alterations, treatment outcomes with regard to cytoreductive surgery, hyperthermic intraperitoneal chemotherapy (HIPEC), and the role of systemic chemotherapy.
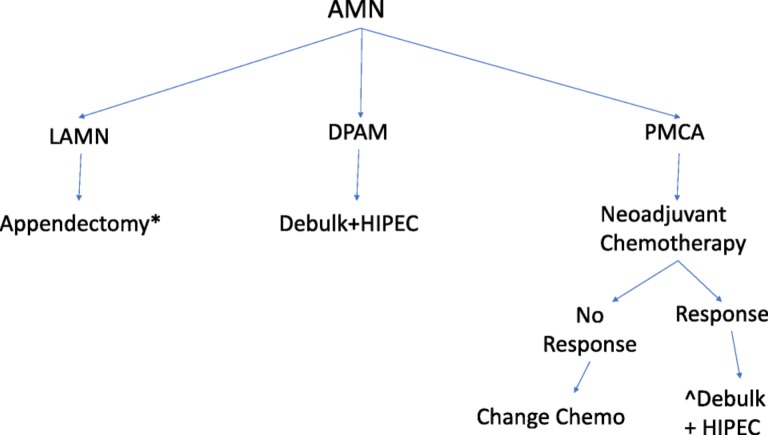
Conclusion: Appendiceal mucinous neoplasms are a heterogeneous group of tumors with a rising incidence. Treatment is based on stage and histology. Low-grade tumors are treated surgically with resection of the primary site in early stage disease, or peritoneal debulking and HIPEC in patients with advanced stage disease. Treatment of high-grade tumors requires further prospective trials, and options include debulking surgery and HIPEC with or without preoperative chemotherapy. Trials evaluating novel therapies based on the molecular profiling of AMN tumors are needed to evaluate therapeutic options in patients who are not surgical candidates.
Implications for practice: This review provides a reference to guide gastroenterologists, pathologists, surgeons, and oncologists in the management of appendiceal mucinous neoplasms (AMNs), a rare and heterogeneous disease with no consensus on histologic classification or guidelines for treatment algorithms. This review summarizes all AMN classifications and proposes a treatment algorithm based on stage and histology of disease.
Keywords: Abdominal surgery; Appendix carcinoma; Review.
© AlphaMed Press 2017.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures


References
-
- McCusker ME, Cote TR, Clegg LX et al. Primary malignant neoplasms of the appendix: A population‐based study from the surveillance, epidemiology and end‐results program, 1973–1998. Cancer 2002;94:3307–3312. - PubMed
-
- Smeenk RM, van Velthuysen ML, Verwaal VJ et al. Appendiceal neoplasms and pseudomyxoma peritonei: A population based study. Eur J Surg Oncol 2008;34:196–201. - PubMed
-
- Rokitansky K, Swaine WE, Sir Sieveking EH, Moore CH, Day GE. A Manual of Pathological Anatomy. Vol. 2 Philadelphia, PA: Blanchard and Lea, 1855;24:100–118.
-
- Carr NJ, McCarthy WF, Sobin LH. Epithelial noncarcinoid tumors and tumor‐like lesions of the appendix. A clinicopathologic study of 184 patients with a multivariate analysis of prognostic factors. Cancer 1995;75:757–768. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
