

Cytomegalovirus Infection in Liver Transplant Recipients: Current Approach to Diagnosis and Management
- PMID: 28663679
- PMCID: PMC5478971
- DOI: 10.1016/j.jceh.2017.05.011
Cytomegalovirus Infection in Liver Transplant Recipients: Current Approach to Diagnosis and Management
Abstract
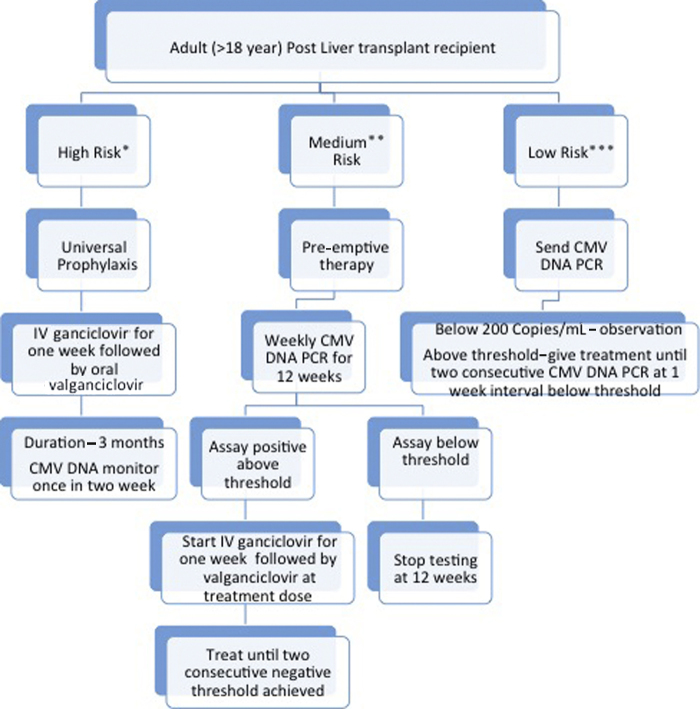
Cytomegalovirus (CMV) infection is the most common viral infection in liver transplant recipients, affecting post-transplant patients and graft survival. Recent advances in diagnosis and management of CMV have led to marked reduction in incidence, severity, and its associated morbidity and mortality. CMV DNA assay is the most commonly used laboratory parameter to diagnose and monitor CMV infection. Current evidence suggests that both pre-emptive and universal prophylaxis approaches are equally justified in liver transplant recipients. Intravenous ganciclovir and oral valganciclovir are the most commonly used drugs for treatment of CMV disease. Most of the centre use valganciclovir prophylaxis for prevention of CMV disease in liver trasplant recipient. The aim of this article is to review the current standard of care for diagnosis and management of CMV disease in liver transplant recipients.
Keywords: CMV disease; CMV, cytomegalovirus; HCV, hepatitis C virus; HHV, human herpes virus; IV, intravenous; LT, liver transplantation; NAT, nucleic acid test; cytomegalovirus; infection; liver transplantation.
Figures
References
-
- Razonable R.R., Paya C.V. Herpesvirus infections in transplant recipients: current challenges in the clinical management of cytomegalovirus and Epstein–Barr virus infections. Herpes J IHMF. 2003;10(3):60–65. - PubMed
-
- Razonable R.R., Emery V.C. 11th Annual Meeting of the IHMF (International Herpes Management Forum). Management of CMV infection and disease in transplant patients. Herpes J IHMF. 2004;11(3):77–86. - PubMed
-
- Gane E., Saliba F., Valdecasas G.J. Randomised trial of efficacy and safety of oral ganciclovir in the prevention of cytomegalovirus disease in liver-transplant recipients. The Oral Ganciclovir International Transplantation Study Group [corrected] Lancet Lond Engl. 1997;350(9093):1729–1733. - PubMed
-
- Ljungman P., Griffiths P., Paya C. Definitions of cytomegalovirus infection and disease in transplant recipients. Clin Infect Dis. 2002;34(8):1094–1097. - PubMed
-
- Razonable R.R., van Cruijsen H., Brown R.A. Dynamics of cytomegalovirus replication during preemptive therapy with oral ganciclovir. J Infect Dis. 2003;187(11):1801–1808. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
