

Endoscopic optical coherence tomography: technologies and clinical applications [Invited]
- PMID: 28663882
- PMCID: PMC5480489
- DOI: 10.1364/BOE.8.002405
Endoscopic optical coherence tomography: technologies and clinical applications [Invited]
Abstract
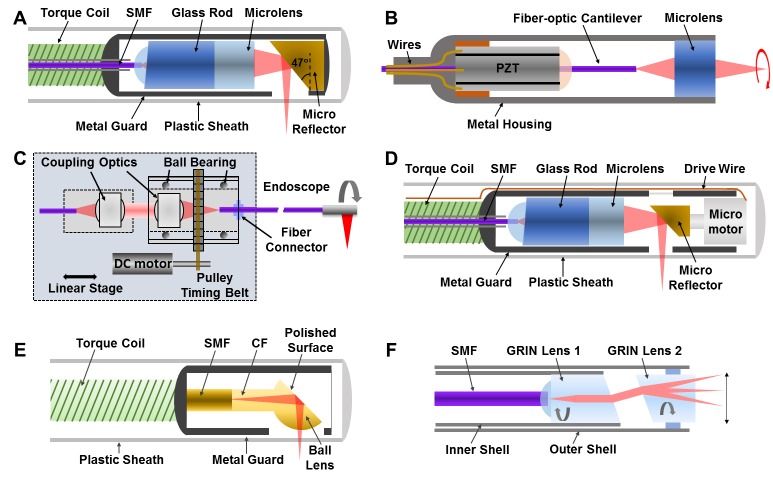
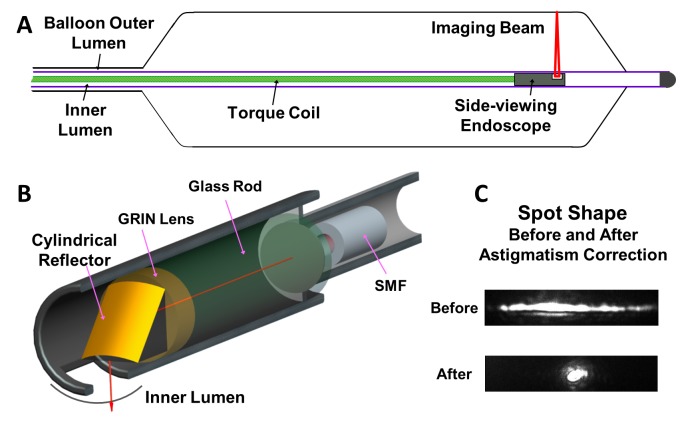
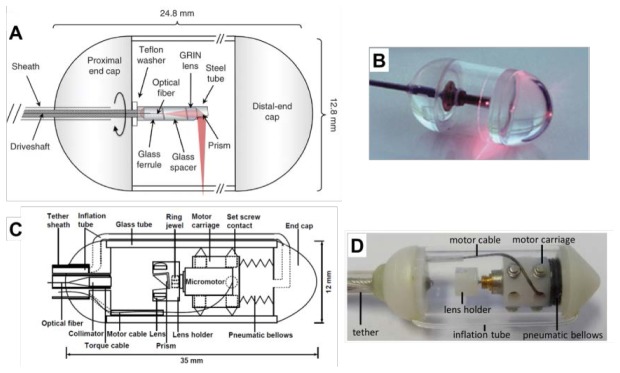
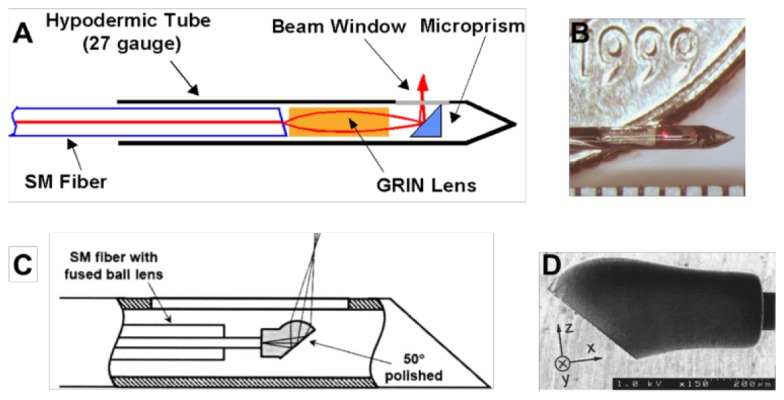
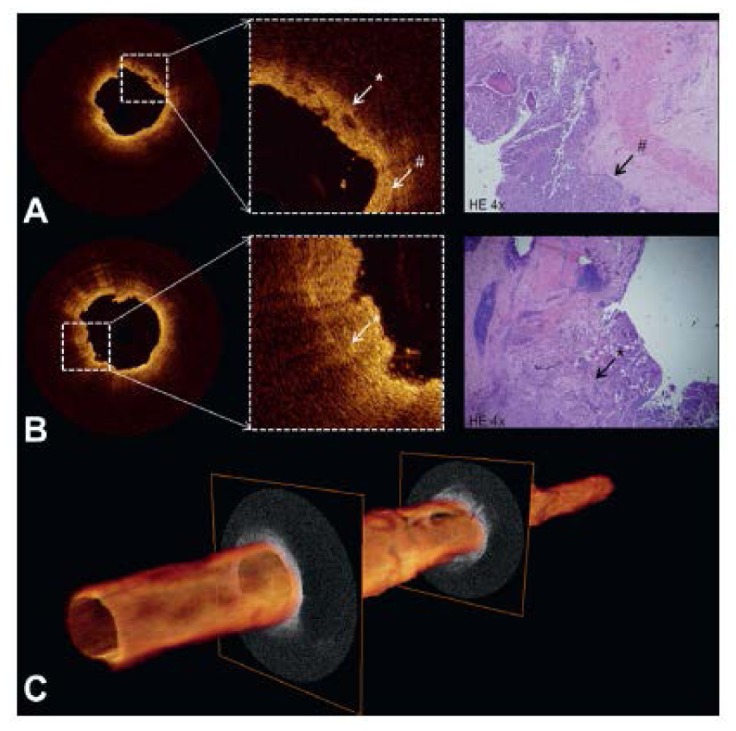
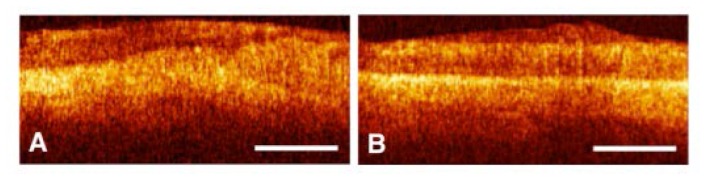
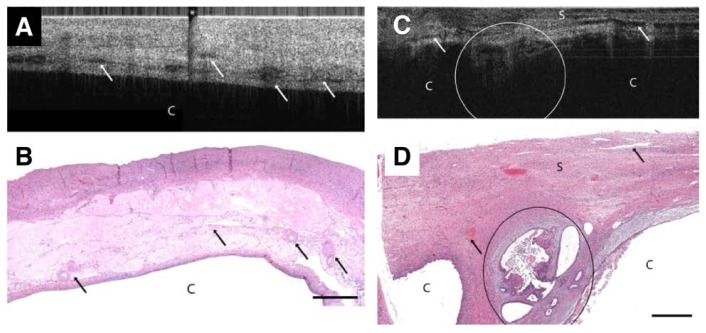
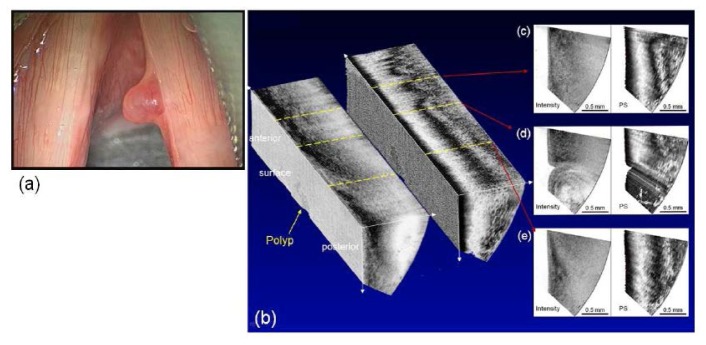
In this paper, we review the current state of technology development and clinical applications of endoscopic optical coherence tomography (OCT). Key design and engineering considerations are discussed for most OCT endoscopes, including side-viewing and forward-viewing probes, along with different scanning mechanisms (proximal-scanning versus distal-scanning). Multi-modal endoscopes that integrate OCT with other imaging modalities are also discussed. The review of clinical applications of endoscopic OCT focuses heavily on diagnosis of diseases and guidance of interventions. Representative applications in several organ systems are presented, such as in the cardiovascular, digestive, respiratory, and reproductive systems. A brief outlook of the field of endoscopic OCT is also discussed.
Keywords: (170.1610) Clinical applications; (170.2150) Endoscopic imaging; (170.4500) Optical coherence tomography; (170.4580) Optical diagnostics for medicine.
Figures
References
-
- Cao T., Tey H. L., “High-definition optical coherence tomography - an aid to clinical practice and research in dermatology,” J. Dtsch. Dermatol. Ges. 13(9), 886–890 (2015). - PubMed
-
- Olsen J., Themstrup L., Jemec G. B., “Optical coherence tomography in dermatology,” G. Ital. Dermatol. Venereol. 150(5), 603–615 (2015). - PubMed
-
- Ulrich M., Themstrup L., de Carvalho N., Manfredi M., Grana C., Ciardo S., Kästle R., Holmes J., Whitehead R., Jemec G. B., Pellacani G., Welzel J., “Dynamic optical coherence tomography in dermatology,” Dermatology (Basel) 232(3), 298–311 (2016). - PubMed
-
- Tearney G. J., Boppart S. A., Bouma B. E., Brezinski M. E., Weissman N. J., Southern J. F., Fujimoto J. G., “Scanning single-mode fiber optic catheter-endoscope for optical coherence tomography,” Opt. Lett. 21(7), 543–545 (1996). - PubMed
-
- Rollins A. M., Ung-Arunyawee R., Chak A., Wong R. C. K., Kobayashi K., Sivak M. V., Jr, Izatt J. A., “Real-time in vivo imaging of human gastrointestinal ultrastructure by use of endoscopic optical coherence tomography with a novel efficient interferometer design,” Opt. Lett. 24(19), 1358–1360 (1999). - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources