

Intracerebral Hemorrhage Caused by Cerebral Hyperperfusion after Superficial Temporal Artery to Middle Cerebral Artery Bypass for Atherosclerotic Occlusive Cerebrovascular Disease
- PMID: 28664022
- PMCID: PMC5364904
- DOI: 10.2176/nmccrj.cr.2016-0043
Intracerebral Hemorrhage Caused by Cerebral Hyperperfusion after Superficial Temporal Artery to Middle Cerebral Artery Bypass for Atherosclerotic Occlusive Cerebrovascular Disease
Abstract
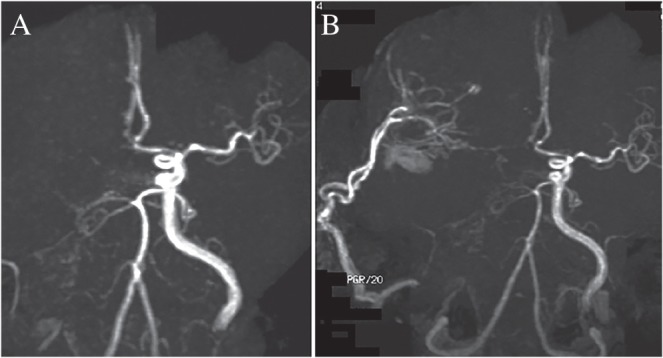
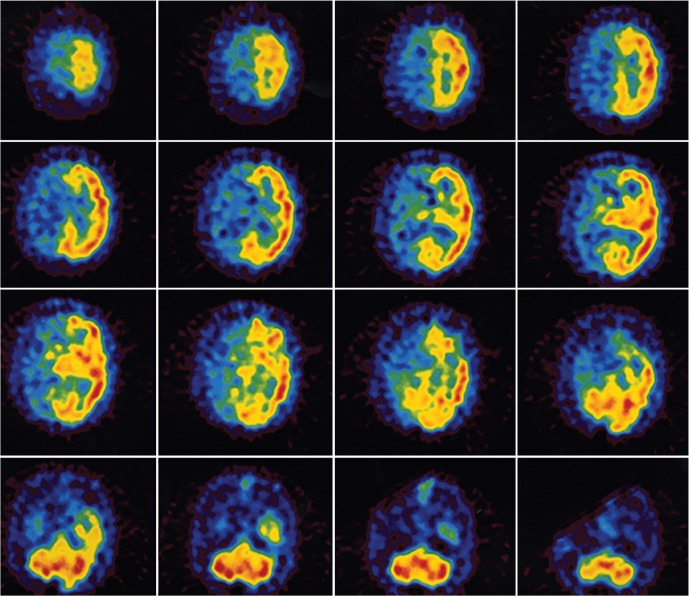
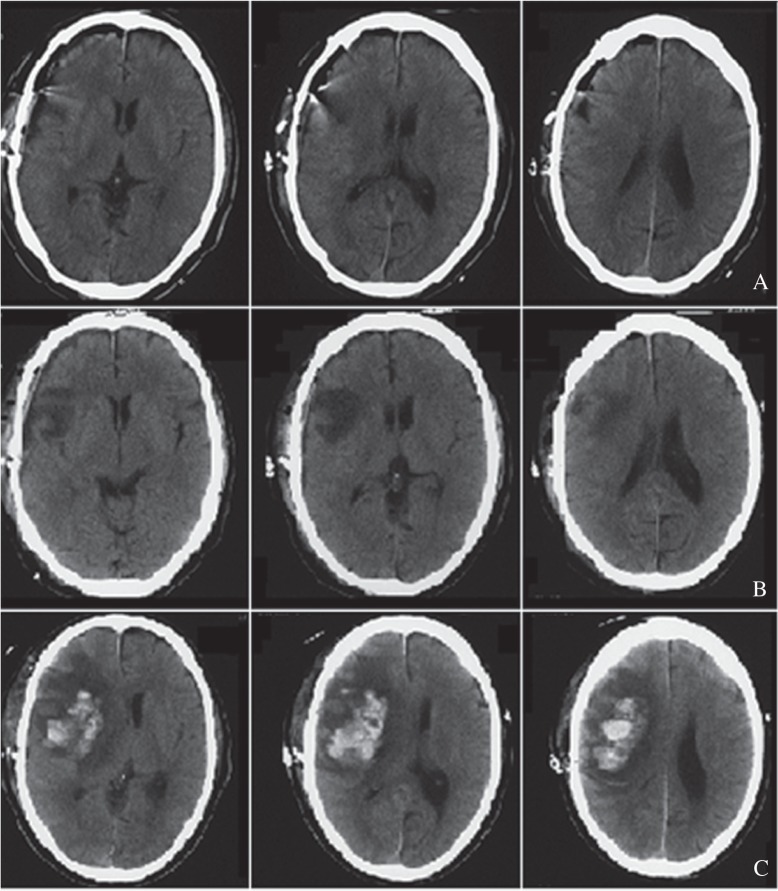
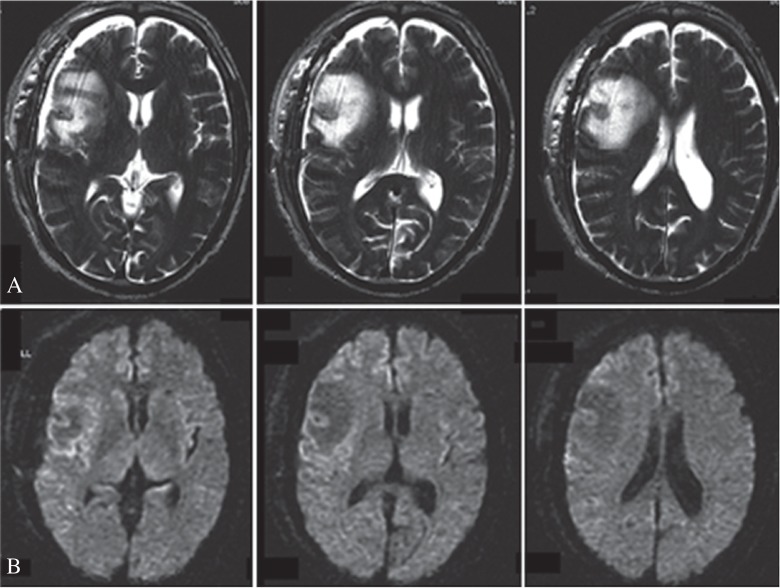
Few papers have reported detailed accounts of intracerebral hemorrhage caused by cerebral hyperperfusion after superficial temporal artery to middle cerebral artery bypass (STA-MCA) bypass for atherosclerotic occlusive cerebrovascular disease. We report a case of vasogenic edema and subsequent intracerebral hemorrhage caused by the cerebral hyperperfusion syndrome (CHS) after STA-MCA bypass for atherosclerotic occlusive cerebrovascular disease disease without intense postoperative blood pressure control. A 63-year-old man with repeating left hemiparesis underwent magnetic resonance angiography (MRA), which revealed right internal carotid artery (ICA) occlusion. We performed a double bypass superficial temporal artery (STA)-middle cerebral artery (MCA) bypass surgery for the M2 and M3 branches. While the patient's postoperative course was relatively uneventful, he suffered generalized convulsions, and computed tomography revealed a low area in the right frontal lobe on Day 4 after surgery. We considered this lesion to be pure vasogenic edema caused by cerebral hyperperfusion after revascularization. Intravenous drip infusion of a free radical scavenger (edaravone) and efforts to reduce systolic blood pressure to <120 mmHg were continued. The patient experienced severe left hemiparesis and disturbance of consciousness on Day 8 after surgery, due to intracerebral hemorrhage in the right frontal lobe at the site of the earlier vasogenic edema. Brain edema associated with cerebral hyperperfusion after STA-MCA bypass for atherosclerotic occlusive cerebrovascular disease should be recognized as a risk factor for intracerebral hemorrhage. The development of brain edema associated with CHS after STA-MCA bypass for atherosclerotic occlusive cerebrovascular disease requires not only intensive control of blood pressure, but also consideration of sedation therapy with propofol.
Keywords: atherosclerotic; cerebral hyperperfusion; extracranial–intracranial bypass; intracerebral hemorrhage.
Conflict of interest statement
Conflicts of Interest Disclosure The authors have no conflicts of interest. All authors who are members of the Japan Neurosurgical Society (JNS) have registered on line Self-reported COI Disclosure Statement Forms through the website for JNS members.
Figures

References
-
- Murai Y, Mizunari T, Takagi R, Amano Y, Mizumura S, Komaba Y, Okubo S, Kobayashi S, Teramoto A: Analysis of ischemic cerebral lesions using 3.0-T diffusion-weighted imaging and magnetic resonance angiography after revascularization surgery for ischemic disease. Clin Neurol Neurosurg 115: 1063– 1070, 2013. - PubMed
-
- Fujimura M, Shimizu H, Inoue T, Mugikura S, Saito A, Tominaga T: Significance of focal cerebral hyperperfusion as a cause of transient neurologic deterioration after extracranial-intracranial bypass for moyamoya disease: comparative study with non-moyamoya patients using N-isopropyl-p-[(123)I]iodoamphetamine single-photon emission computed tomography. Neurosurgery 68: 957– 964, 2011. - PubMed
-
- Hosoda K, Kawaguchi T, Ishii K, Minoshima S, Shibata Y, Iwakura M, Ishiguro S, Kohmura E: Prediction of hyperperfusion after carotid endarterectomy by brain SPECT analysis with semiquantitative statistical mapping method. Stroke 34: 1187– 1193, 2003. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous