

Predicting the response to CTLA-4 blockade by longitudinal noninvasive monitoring of CD8 T cells
- PMID: 28666979
- PMCID: PMC5551571
- DOI: 10.1084/jem.20161950
Predicting the response to CTLA-4 blockade by longitudinal noninvasive monitoring of CD8 T cells
Abstract
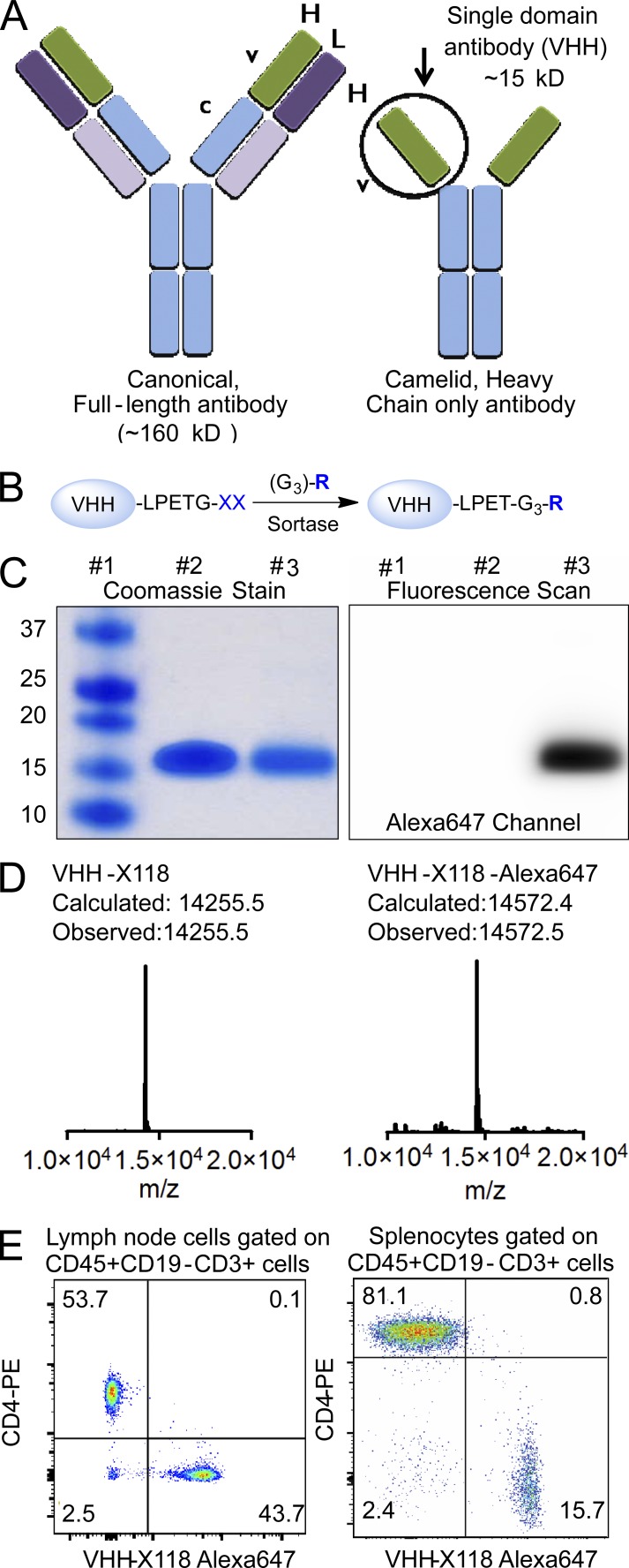
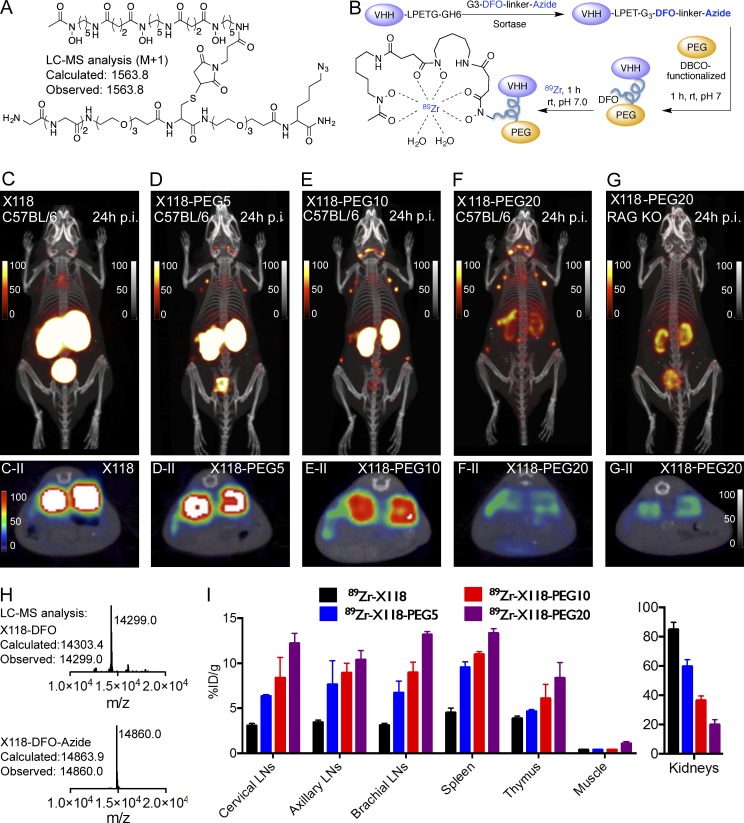
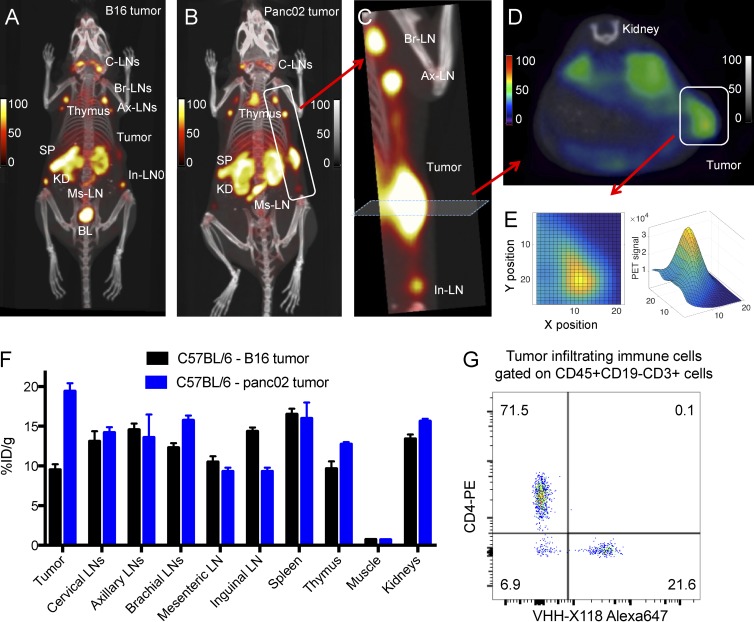
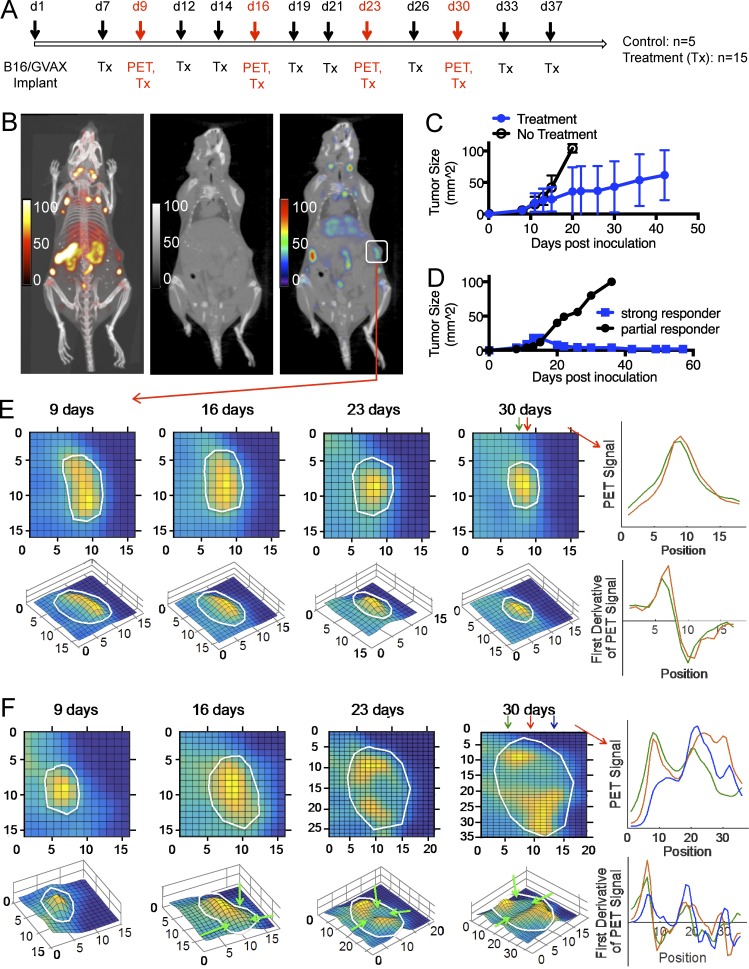
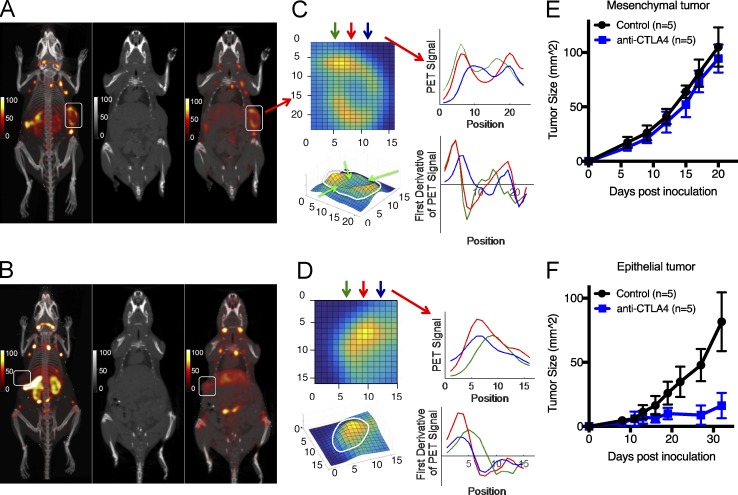
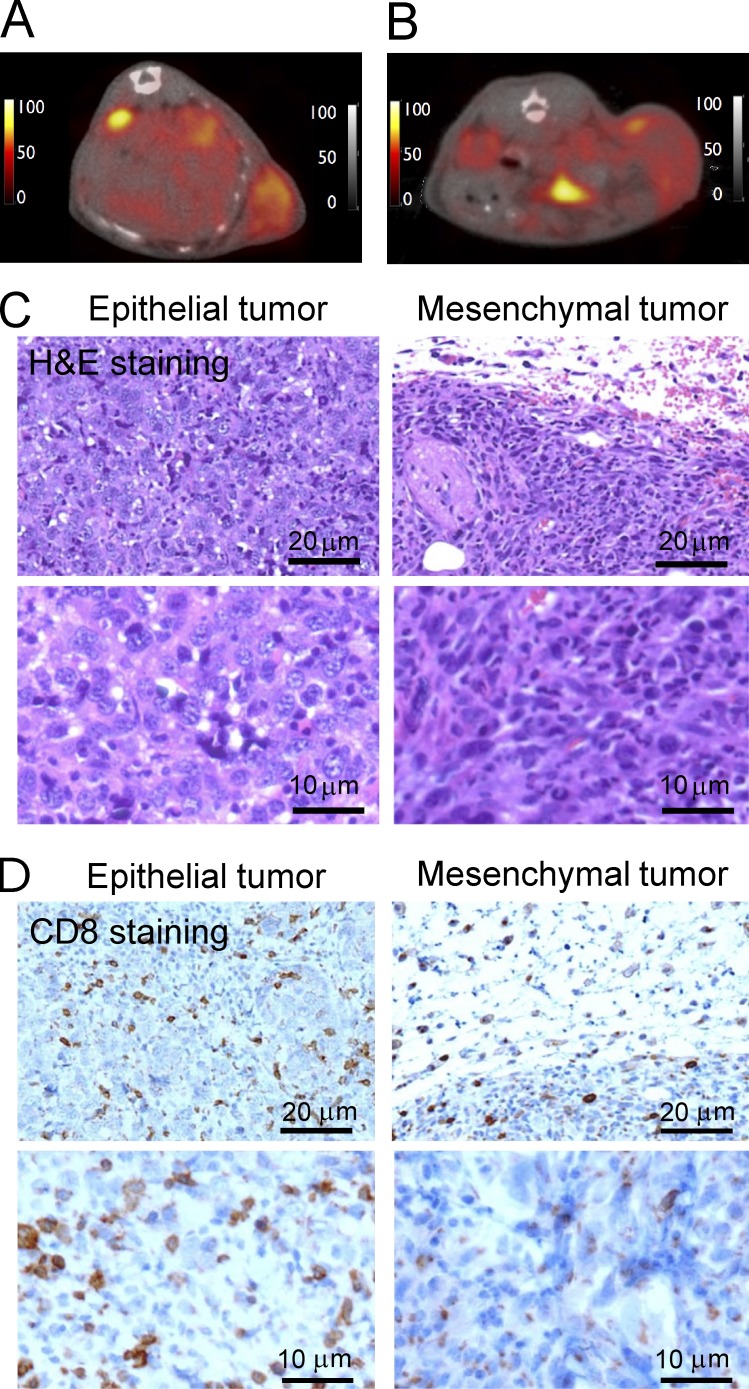
Immunotherapy using checkpoint-blocking antibodies against targets such as CTLA-4 and PD-1 can cure melanoma and non-small cell lung cancer in a subset of patients. The presence of CD8 T cells in the tumor correlates with improved survival. We show that immuno-positron emission tomography (immuno-PET) can visualize tumors by detecting infiltrating lymphocytes and, through longitudinal observation of individual animals, distinguish responding tumors from those that do not respond to therapy. We used 89Zr-labeled PEGylated single-domain antibody fragments (VHHs) specific for CD8 to track the presence of intratumoral CD8+ T cells in the immunotherapy-susceptible B16 melanoma model in response to checkpoint blockade. A 89Zr-labeled PEGylated anti-CD8 VHH detected thymus and secondary lymphoid structures as well as intratumoral CD8 T cells. Animals that responded to CTLA-4 therapy showed a homogeneous distribution of the anti-CD8 PET signal throughout the tumor, whereas more heterogeneous infiltration of CD8 T cells correlated with faster tumor growth and worse responses. To support the validity of these observations, we used two different transplantable breast cancer models, yielding results that conformed with predictions based on the antimelanoma response. It may thus be possible to use immuno-PET and monitor antitumor immune responses as a prognostic tool to predict patient responses to checkpoint therapies.
© 2017 Rashidian et al.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
