

Digoxin Use and Subsequent Clinical Outcomes in Patients With Atrial Fibrillation With or Without Heart Failure in the ENGAGE AF-TIMI 48 Trial
- PMID: 28666993
- PMCID: PMC5586309
- DOI: 10.1161/JAHA.117.006035
Digoxin Use and Subsequent Clinical Outcomes in Patients With Atrial Fibrillation With or Without Heart Failure in the ENGAGE AF-TIMI 48 Trial
Abstract
Background: Digoxin is widely used in patients with atrial fibrillation despite the lack of randomized controlled trials. Observational studies report conflicting results regarding its association with mortality, perhaps because of residual confounding by the presence of heart failure (HF).
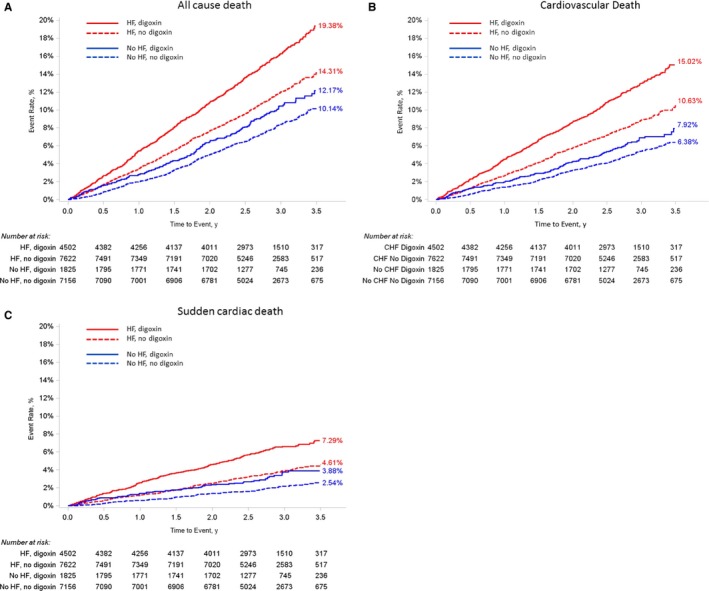
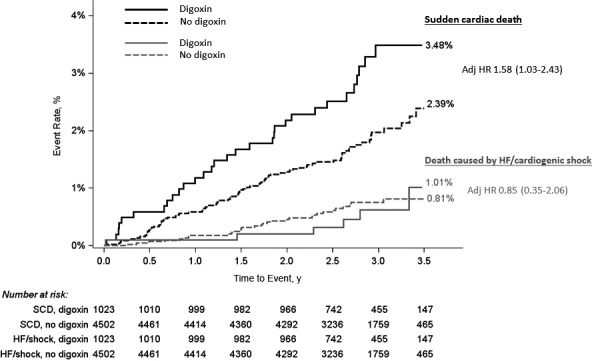
Methods and results: In the ENGAGE AF-TIMI 48 (Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48) trial, clinical outcomes of patients with atrial fibrillation with and without HF were examined by baseline digoxin use during a median follow-up of 2.8 years. HF was defined at baseline as prior or current clinical stage C or D HF. Of 21 105 patients enrolled, 6327 (30%) were treated with digoxin at baseline. Among patients without HF (n=8981), digoxin use (20%) was independently associated with sudden cardiac death (adjusted hazard ratio, 1.51; 95% CI, 1.10-2.08), with no significant interaction by age, sex, left ventricular ejection fraction, renal function, or concomitant medications (P>0.05 for each). Consistent results were observed using propensity matching (adjusted hazard ratio for sudden cardiac death, 1.90; 95% CI, 1.36-2.65). Among patients with HF (n=12 124), digoxin use (37%) was associated with an increase in all-cause death, cardiovascular death, sudden cardiac death, and death caused by HF/cardiogenic shock (P<0.01 for each), but not with noncardiovascular death, stroke/systemic embolism, or myocardial infarction.
Conclusions: In this observational analysis of patients with atrial fibrillation without investigator-reported HF, digoxin use was significantly associated with sudden cardiac death. While residual confounding cannot be excluded, the association between digoxin use and worse clinical outcomes highlights the need to examine digoxin use, particularly when prescribed to control heart rate in patients with atrial fibrillation in a randomized trial.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00781391.
Keywords: atrial fibrillation; digoxin; heart failure; mortality; sudden cardiac death.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Washam JB, Stevens SR, Lokhnygina Y, Halperin JL, Breithardt G, Singer DE, Mahaffey KW, Hankey GJ, Berkowitz SD, Nessel CC, Fox KA, Califf RM, Piccini JP, Patel MR; ROCKET AF Steering Committee and Investigators . Digoxin use in patients with atrial fibrillation and adverse cardiovascular outcomes: a retrospective analysis of the rivaroxaban once daily oral direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation (ROCKET AF). Lancet. 2015;385:2363–2370. - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW; ACC/AHA Task Force Members . 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–2104. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P; Authors/Task Force Members; Document Reviewers . 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS: the Task Force for the management of atrial fibrillation of the European Society of Cardiology (ESC). Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Endorsed by the European Stroke Organisation (ESO). Eur Heart J. 2016;37:2893–2962.
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1–e76. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
