

Associations between maternal size and health outcomes for women undergoing caesarean section: a multicentre prospective observational study (The MUM SIZE Study)
- PMID: 28667219
- PMCID: PMC5734348
- DOI: 10.1136/bmjopen-2016-015630
Associations between maternal size and health outcomes for women undergoing caesarean section: a multicentre prospective observational study (The MUM SIZE Study)
Abstract
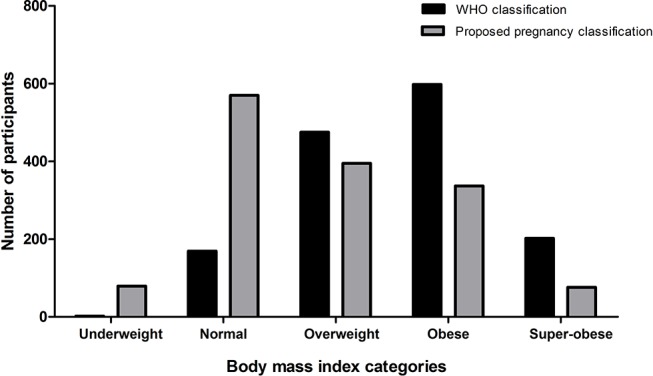
Objectives: To investigate associations between maternal body mass index (BMI) at delivery (using pregnancy-specific BMI cut-off values 5 kg/m2 higher in each of the WHO groups) and clinical, theatre utilisation and health economic outcomes for women undergoing caesarean section (CS).
Design: A prospective multicentre observational study.
Setting: Seven secondary or tertiary referral obstetric hospitals.
Participants: One thousand and four hundred and fifty-seven women undergoing all categories of CS.
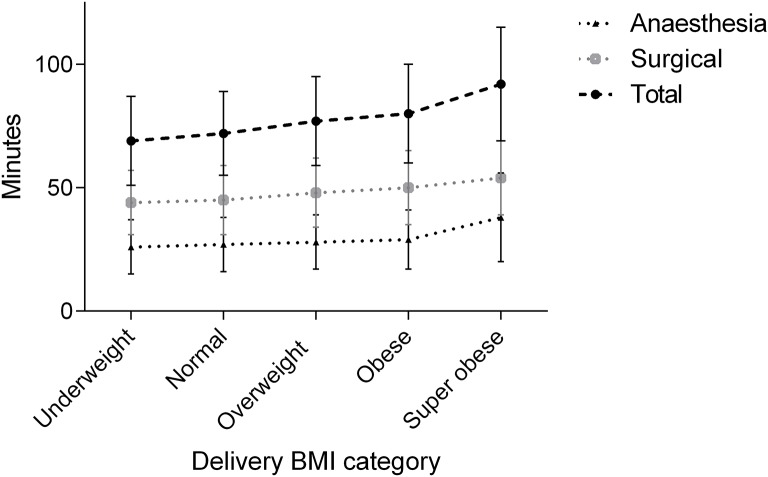
Data collection: Height and weight were recorded at the initial antenatal visit and at delivery. We analysed the associations between delivery BMI (continuous and pregnancy-specific cut-off values) and total theatre time, surgical time, anaesthesia time, maternal and neonatal adverse outcomes, total hospital admission and theatre costs.
Results: Mean participant characteristics were: age 32 years, gestation at delivery 38.4 weeks and delivery BMI 32.2 kg/m2. Fifty-five per cent of participants were overweight, obese or super-obese using delivery pregnancy-specific BMI cut-off values. As BMI increased, total theatre time, surgical time and anaesthesia time increased. Super-obese participants had approximately 27% (17 min, p<0.001) longer total theatre time, 20% (9 min, p<0.001), longer surgical time and 40% (11 min, p<0.001) longer anaesthesia time when compared with normal BMI participants. Increased BMI at delivery was associated with increased risk of maternal intensive care unit admission (relative risk 1.07, p=0.045), but no increased risk of neonatal admission to higher acuity care. Total hospital admission costs were 15% higher in super-obese women compared with normal BMI women and theatre costs were 27% higher in super-obese women.
Conclusions: Increased maternal BMI was associated with increased total theatre time, surgical and anaesthesia time, increased total hospital admission costs and theatre costs. Clinicians and health administrators should consider these clinical risks, time implications and financial costs when managing pregnant women.
Keywords: Health economics; Quality in health care; caesarean section; obesity.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization classification of Body Mass Index. http://apps.who.int/bmi/index.jsp?introPage=intro_3.html (accessed 23 Aug 2015).
-
- Cantwell R, Clutton-Brock T, Cooper G, et al. . Saving mothers' lives: reviewing maternal deaths to make motherhood safer: 2006-2008. The eighth report of the confidential enquiries into maternal deaths in the United Kingdom. BJOG 2011;118(Suppl 1):1–203. 10.1111/j.1471-0528.2010.02847.x - DOI - PubMed
-
- Lewis G. The Confidential Enquiry into Maternal and Child Health(CEMACH). Saving mothers' Lives:reviewing maternal deaths to make motherhood safer - 2003-2005. London: CEMACH, 2007.
-
- Knight M, Kenyon S, Brocklehurst P, et al. . Saving lives, improving mothers’ Care - Lessons learned to inform future maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2009–12. Oxford: National Perinatal Epidemiology Unit, University of Oxford, 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials