

The Effect of Adding Comorbidities to Current Centers for Disease Control and Prevention Central-Line-Associated Bloodstream Infection Risk-Adjustment Methodology
- PMID: 28669363
- PMCID: PMC5711399
- DOI: 10.1017/ice.2017.129
The Effect of Adding Comorbidities to Current Centers for Disease Control and Prevention Central-Line-Associated Bloodstream Infection Risk-Adjustment Methodology
Abstract
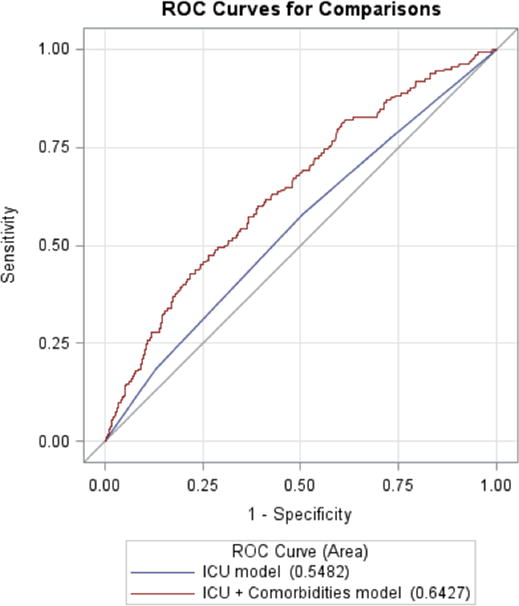
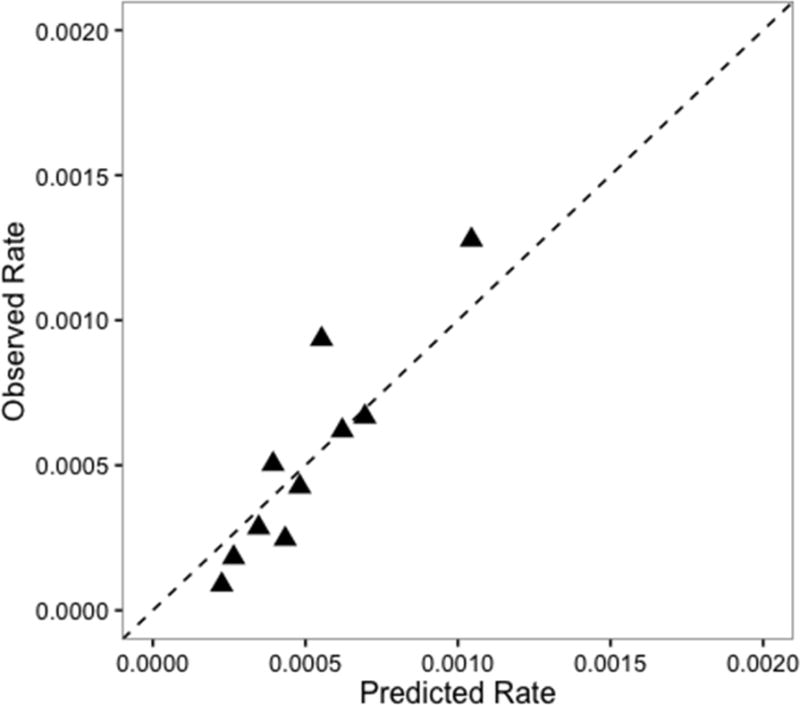
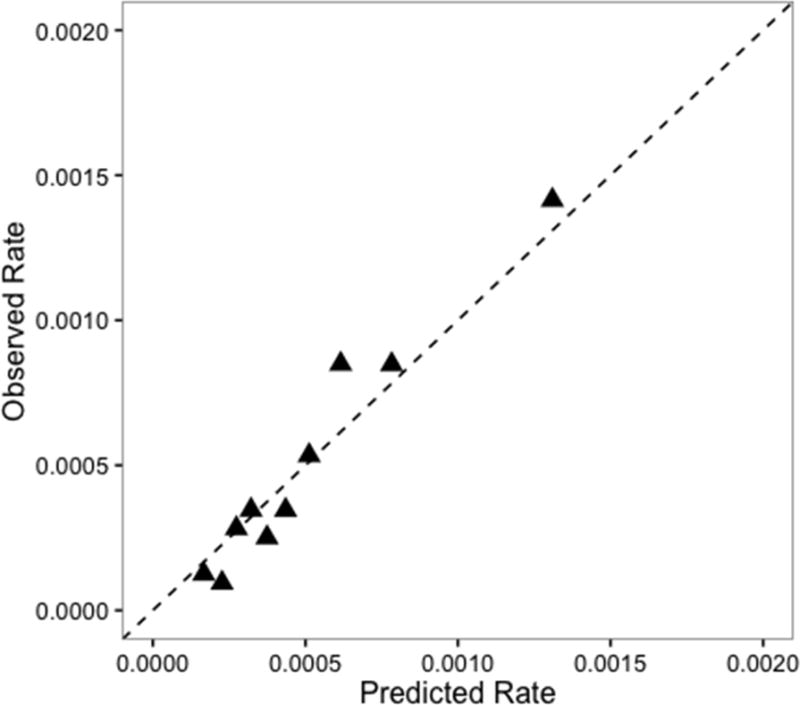
BACKGROUND Risk adjustment is needed to fairly compare central-line-associated bloodstream infection (CLABSI) rates between hospitals. Until 2017, the Centers for Disease Control and Prevention (CDC) methodology adjusted CLABSI rates only by type of intensive care unit (ICU). The 2017 CDC models also adjust for hospital size and medical school affiliation. We hypothesized that risk adjustment would be improved by including patient demographics and comorbidities from electronically available hospital discharge codes. METHODS Using a cohort design across 22 hospitals, we analyzed data from ICU patients admitted between January 2012 and December 2013. Demographics and International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) discharge codes were obtained for each patient, and CLABSIs were identified by trained infection preventionists. Models adjusting only for ICU type and for ICU type plus patient case mix were built and compared using discrimination and standardized infection ratio (SIR). Hospitals were ranked by SIR for each model to examine and compare the changes in rank. RESULTS Overall, 85,849 ICU patients were analyzed and 162 (0.2%) developed CLABSI. The significant variables added to the ICU model were coagulopathy, paralysis, renal failure, malnutrition, and age. The C statistics were 0.55 (95% CI, 0.51-0.59) for the ICU-type model and 0.64 (95% CI, 0.60-0.69) for the ICU-type plus patient case-mix model. When the hospitals were ranked by adjusted SIRs, 10 hospitals (45%) changed rank when comorbidity was added to the ICU-type model. CONCLUSIONS Our risk-adjustment model for CLABSI using electronically available comorbidities demonstrated better discrimination than did the CDC model. The CDC should strongly consider comorbidity-based risk adjustment to more accurately compare CLABSI rates across hospitals. Infect Control Hosp Epidemiol 2017;38:1019-1024.
Conflict of interest statement
The authors have no other conflicts of interest to disclose.
Figures
Comment in
-
Moving to a More Level Playing Field: The Need for Risk Adjustment of Publicly Reported Hospital CLABSI Performance.Infect Control Hosp Epidemiol. 2017 Sep;38(9):1025-1026. doi: 10.1017/ice.2017.159. Infect Control Hosp Epidemiol. 2017. PMID: 28840794 No abstract available.
References
-
- Stevens V, Geiger K, Concannon C, Nelson RE, Brown J, Dumyati G. Inpatient costs, mortality and 30-day re-admission in patients with central-line-associated bloodstream infections. Clin Microbiol Infect. 2014;20(5):O318–24. - PubMed
-
- Centers for Disease Control and Prevention (CDC) National and state healthcare-associated infections standardized infection ratio report: Using data reported to the national healthcare safety network. 2012
-
- Centers for Disease Control and Prevention (CDC) The NHSN guide to the standardized infection ratio: A guide to the SIR. 2016
-
- Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. - PubMed
-
- Allison P. Discrete-time methods for the analysis of event histories. Sociological Methodology. 1982;13:61–98.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
