

Splenial Lesions of the Corpus Callosum: Disease Spectrum and MRI Findings
- PMID: 28670166
- PMCID: PMC5447647
- DOI: 10.3348/kjr.2017.18.4.710
Splenial Lesions of the Corpus Callosum: Disease Spectrum and MRI Findings
Abstract
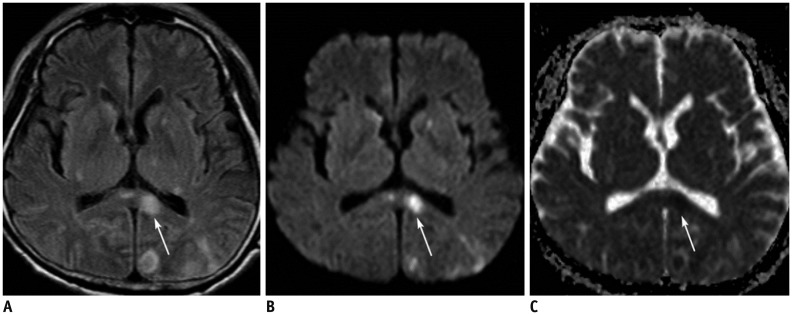
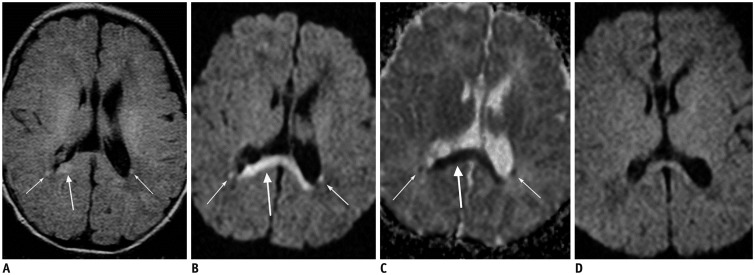
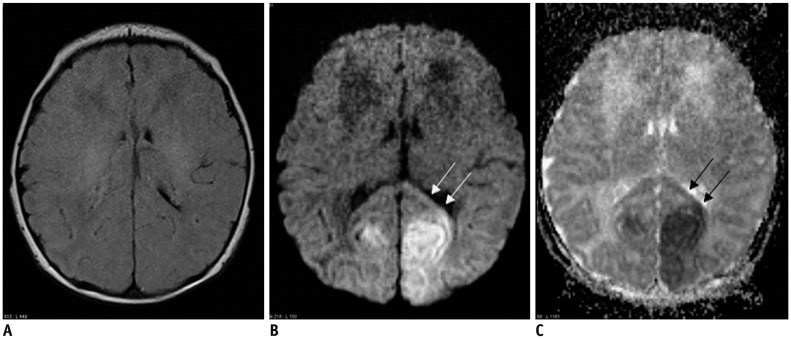
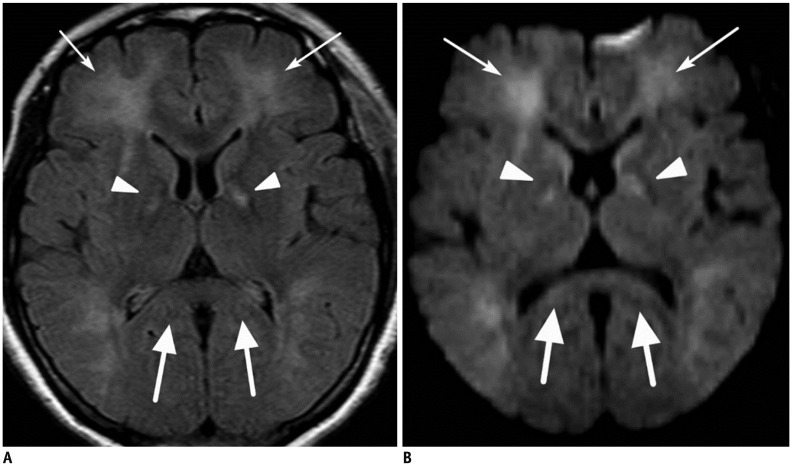
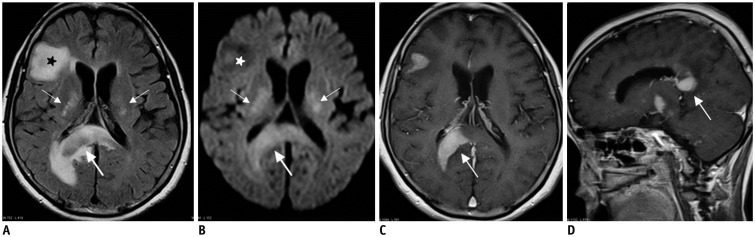
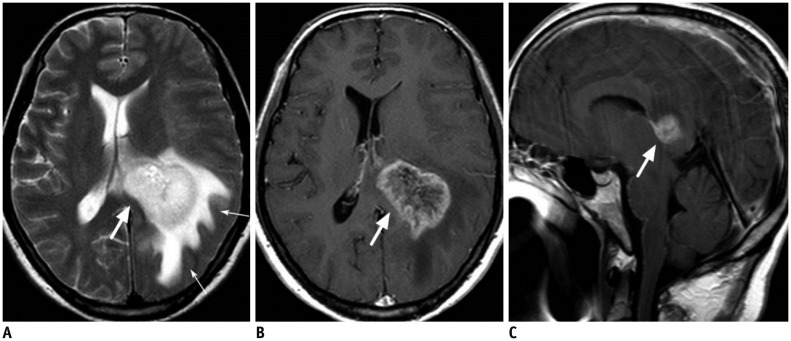
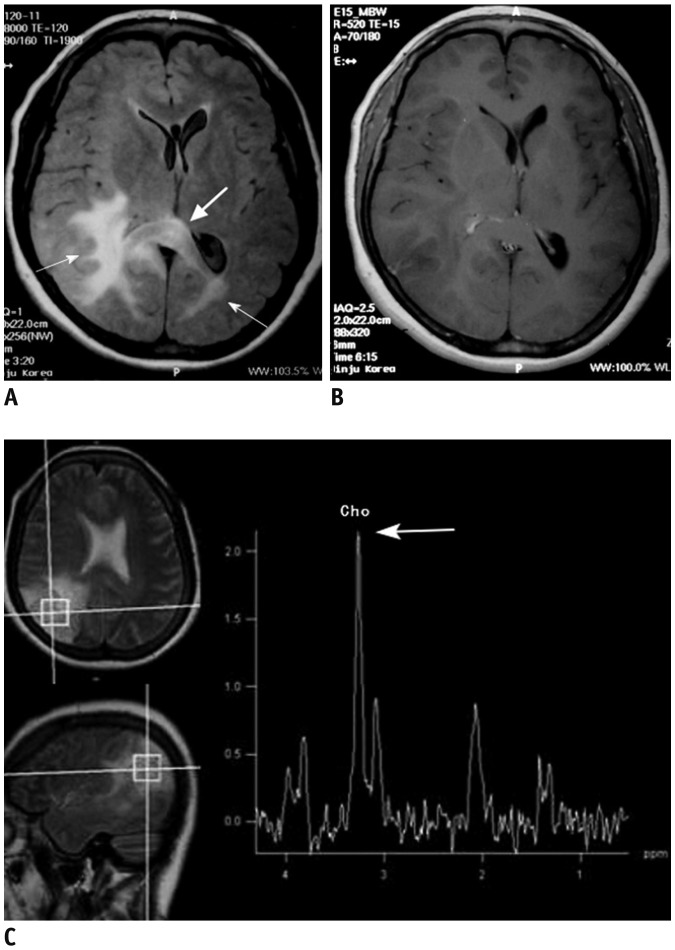
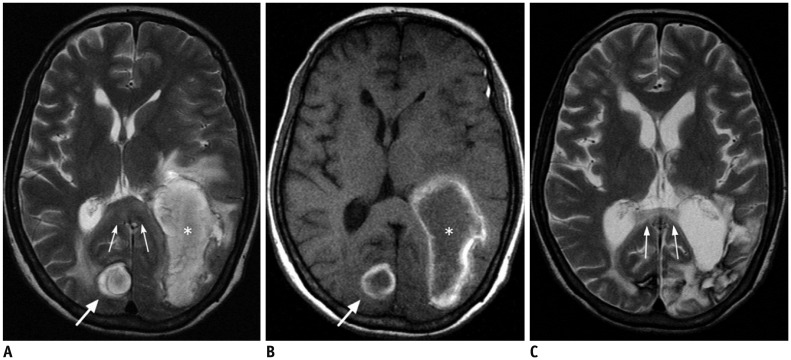
The corpus callosum (CC) is the largest white matter structure in the brain, consisting of more than 200-250 million axons that provide a large connection mainly between homologous cerebral cortical areas in mirror image sites. The posterior end of the CC is the thickest part, which is called the splenium. Various diseases including congenital to acquired lesions including congenital anomalies, traumatic lesions, ischemic diseases, tumors, metabolic, toxic, degenerative, and demyelinating diseases, can involve the splenium of the CC and their clinical symptoms and signs are also variable. Therefore, knowledge of the disease entities and the imaging findings of lesions involving the splenium is valuable in clinical practice. MR imaging is useful for the detection and differential diagnosis of splenial lesions of the CC. In this study, we classify the disease entities and describe imaging findings of lesions involving the splenium of the CC based on our experiences and a review of the literature.
Keywords: Brain; Corpus callosum; Magnetic resonance imaging.
Figures

References
-
- Lee SK, Kim DI, Kim J, Kim DJ, Kim HD, Kim DS, et al. Diffusion-tensor MR imaging and fiber tractography: a new method of describing aberrant fiber connections in developmental CNS anomalies. Radiographics. 2005;25:53–65. discussion 66-68. - PubMed
-
- Doherty MJ, Jayadev S, Watson NF, Konchada RS, Hallam DK. Clinical implications of splenium magnetic resonance imaging signal changes. Arch Neurol. 2005;62:433–437. - PubMed
-
- Park MK, Hwang SH, Jung S, Hong SS, Kwon SB. Lesions in the splenium of the corpus callosum: clinical and radiological implications. Neurol Asia. 2014;19:79–88.
-
- Georgy BA, Hesselink JR, Jernigan TL. MR imaging of the corpus callosum. AJR Am J Roentgenol. 1993;160:949–955. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
