

Neurocognitive Functioning of Children Treated for High-Risk B-Acute Lymphoblastic Leukemia Randomly Assigned to Different Methotrexate and Corticosteroid Treatment Strategies: A Report From the Children's Oncology Group
- PMID: 28671857
- PMCID: PMC5549456
- DOI: 10.1200/JCO.2016.71.7587
Neurocognitive Functioning of Children Treated for High-Risk B-Acute Lymphoblastic Leukemia Randomly Assigned to Different Methotrexate and Corticosteroid Treatment Strategies: A Report From the Children's Oncology Group
Abstract
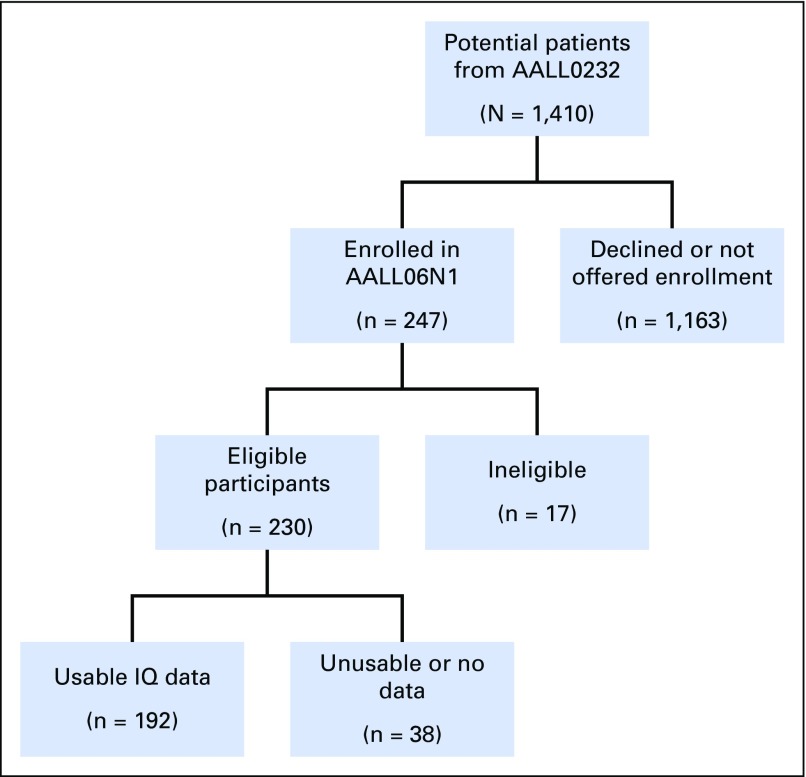
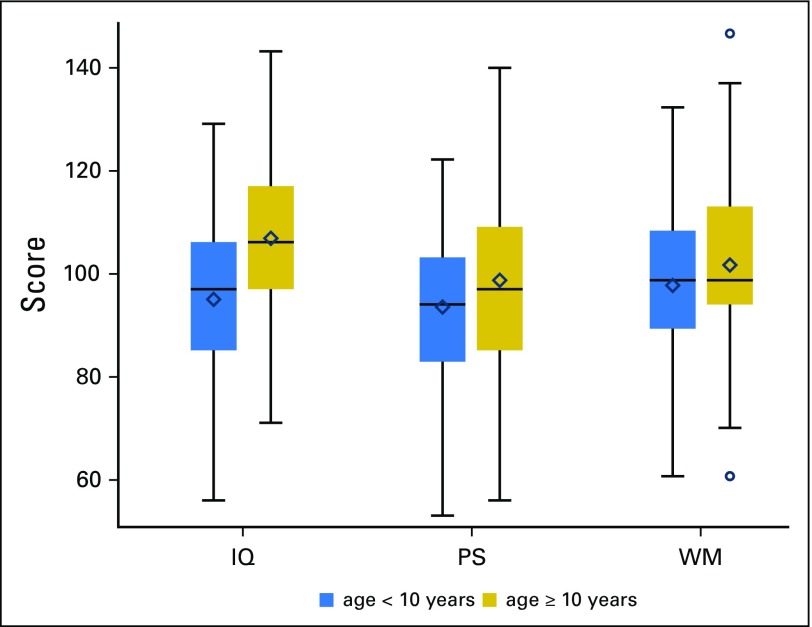
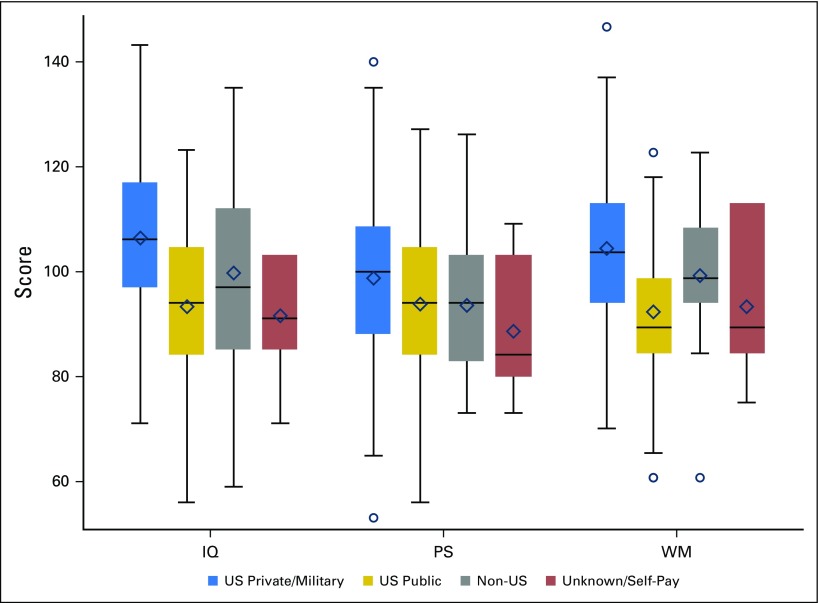
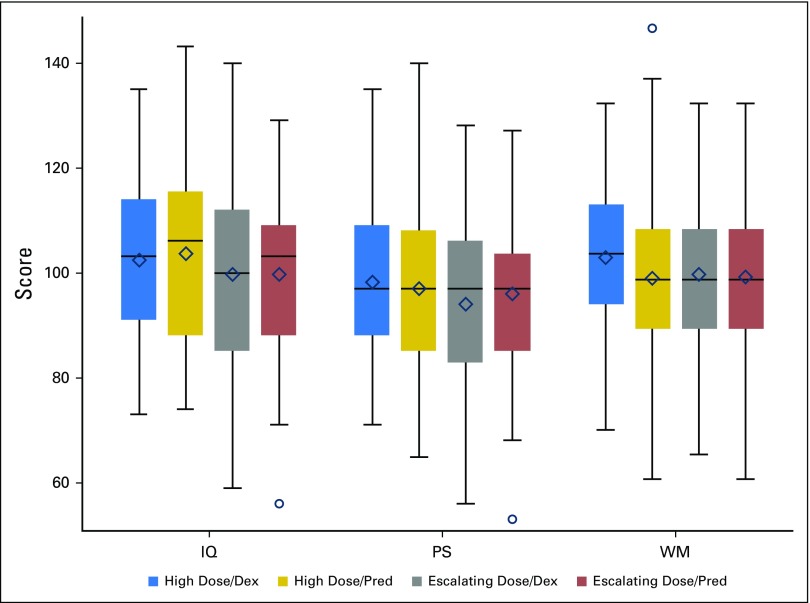
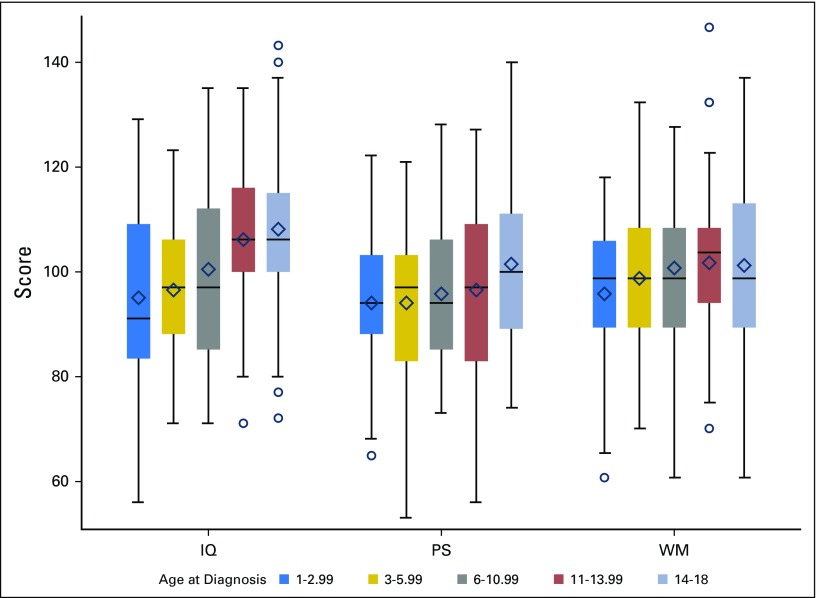
Purpose Survivors of childhood acute lymphoblastic leukemia (ALL) are at risk for neurocognitive deficits that are associated with treatment, individual, and environmental factors. This study examined the impact of different methotrexate (MTX) and corticosteroid treatment strategies on neurocognitive functioning in children with high-risk B-lineage ALL. Methods Participants were randomly assigned to receive high-dose MTX with leucovorin rescue or escalating dose MTX with PEG asparaginase without leucovorin rescue. Patients were also randomly assigned to corticosteroid therapy that included either dexamethasone or prednisone. A neurocognitive evaluation of intellectual functioning (IQ), working memory, and processing speed (PS) was conducted 8 to 24 months after treatment completion (n = 192). Results The method of MTX delivery and corticosteroid assignment were unrelated to differences in neurocognitive outcomes after controlling for ethnicity, race, age, gender, insurance status, and time off treatment; however, survivors who were age < 10 years at diagnosis (n = 89) had significantly lower estimated IQ ( P < .001) and PS scores ( P = .02) compared with participants age ≥ 10 years. In addition, participants who were covered by US public health insurance had estimated IQs that were significantly lower ( P < .001) than those with US private or military insurance. Conclusion Children with high-risk B-lineage ALL who were age < 10 years at diagnosis are at risk for deficits in IQ and PS in the absence of cranial radiation, regardless of MTX delivery or corticosteroid type. These data may serve as a basis for developing screening protocols to identify children who are at high risk for deficits so that early intervention can be initiated to mitigate the impact of therapy on neurocognitive outcomes.
Figures
Comment in
-
Neurocognitive Functioning in the AALL0232 Protocol.J Clin Oncol. 2017 Dec 10;35(35):3989. doi: 10.1200/JCO.2017.75.1453. Epub 2017 Oct 18. J Clin Oncol. 2017. PMID: 29045161 No abstract available.
-
Reply to I.J. Cohen.J Clin Oncol. 2017 Dec 10;35(35):3989-3991. doi: 10.1200/JCO.2017.75.7252. Epub 2017 Oct 18. J Clin Oncol. 2017. PMID: 29045162 No abstract available.
References
-
- Campbell LK, Scaduto M, Sharp W, et al. : A meta-analysis of the neurocognitive sequelae of treatment for childhood acute lymphocytic leukemia. Pediatr Blood Cancer 49:65-73, 2007 - PubMed
-
- Mennes M, Stiers P, Vandenbussche E, et al. : Attention and information processing in survivors of childhood acute lymphoblastic leukemia treated with chemotherapy only. Pediatr Blood Cancer 44:478-486, 2005 - PubMed
-
- Peterson CC, Johnson CE, Ramirez LY, et al. : A meta-analysis of the neuropsychological sequelae of chemotherapy-only treatment for pediatric acute lymphoblastic leukemia. Pediatr Blood Cancer 51:99-104, 2008 - PubMed
-
- Knight S, McCarthy M, Anderson V, et al. : Visuomotor function in children treated for acute lymphoblastic leukaemia with chemotherapy only. Dev Neuropsychol 39:101-112, 2014 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
