

Development of the Barriers to Error Disclosure Assessment Tool
- PMID: 28671908
- PMCID: PMC5748022
- DOI: 10.1097/PTS.0000000000000331
Development of the Barriers to Error Disclosure Assessment Tool
Abstract
Objectives: An interprofessional group of health colleges' faculty created and piloted the Barriers to Error Disclosure Assessment tool as an instrument to measure barriers to medical error disclosure among health care providers.
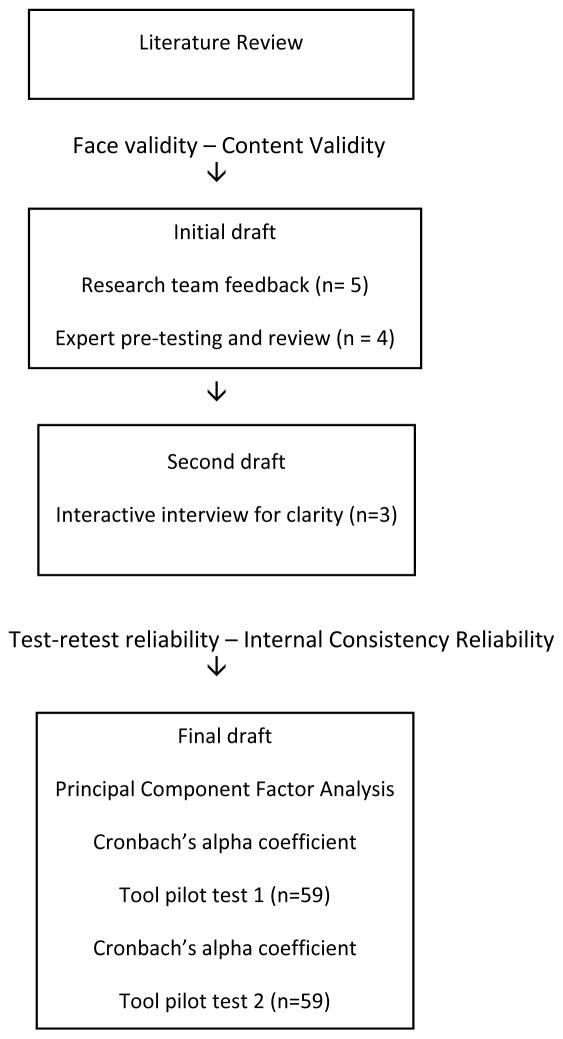
Methods: A review of the literature guided the creation of items describing influences on the decision to disclose a medical error. Local and national experts in error disclosure used a modified Delphi process to gain consensus on the items included in the pilot. After receiving university institutional review board approval, researchers distributed the tool to a convenience sample of physicians (n = 19), pharmacists (n = 20), and nurses (n = 20) from an academic medical center. Means and SDs were used to describe the sample. Intraclass correlation coefficients were used to examine test-retest correspondence between the continuous items on the scale. Factor analysis with varimax rotation was used to determine factor loadings and examine internal consistency reliability. Cronbach α coefficients were calculated during initial and subsequent administrations to assess test-retest reliability.
Results: After omitting 2 items with intraclass correlation coefficient of less than 0.40, intraclass correlation coefficients ranged from 0.43 to 0.70, indicating fair to good test-retest correspondence between the continuous items on the final draft. Factor analysis revealed the following factors during the initial administration: confidence and knowledge barriers, institutional barriers, psychological barriers, and financial concern barriers to medical error disclosure. α Coefficients of 0.85 to 0.93 at time 1 and 0.82 to 0.95 at time 2 supported test-retest reliability.
Conclusions: The final version of the 31-item tool can be used to measure perceptions about abilities for disclosing, impressions regarding institutional policies and climate, and specific barriers that inhibit disclosure by health care providers. Preliminary evidence supports the tool's validity and reliability for measuring disclosure variables.
Copyright © 2017 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflict of interest.
Figures
References
-
- James JT. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf. 2013;9(3):122–128. - PubMed
-
- National Quality Forum (NQF) Safe practices for better healthcare-2010 update: A consensus report. Washington, DC: NQF; 2010. [Accessed 6/28/16]. http://www.qualityforum.org/Publications/2010/04/Safe_Practices_for_Bett....
-
- Commission, TJ. Hospital Accreditation Standards, 2007. Oakbrook Terrace, Il: Joint Commission Resources; 2007.
-
- Institute of Medicine (IOM) To err is human: building a safer health system. Washington, DC: National Academy Press; 1999.
-
- Gallagher TH, Waterman AD, Ebers AG, et al. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA. 2003;289:1001–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
