

Effects of an Intervention to Reduce Hospitalizations From Nursing Homes: A Randomized Implementation Trial of the INTERACT Program
- PMID: 28672291
- PMCID: PMC5710568
- DOI: 10.1001/jamainternmed.2017.2657
Effects of an Intervention to Reduce Hospitalizations From Nursing Homes: A Randomized Implementation Trial of the INTERACT Program
Abstract
Importance: Medicare payment initiatives are spurring efforts to reduce potentially avoidable hospitalizations.
Objective: To determine whether training and support for implementation of a nursing home (NH) quality improvement program (Interventions to Reduce Acute Care Transfers [INTERACT]) reduced hospital admissions and emergency department (ED) visits.
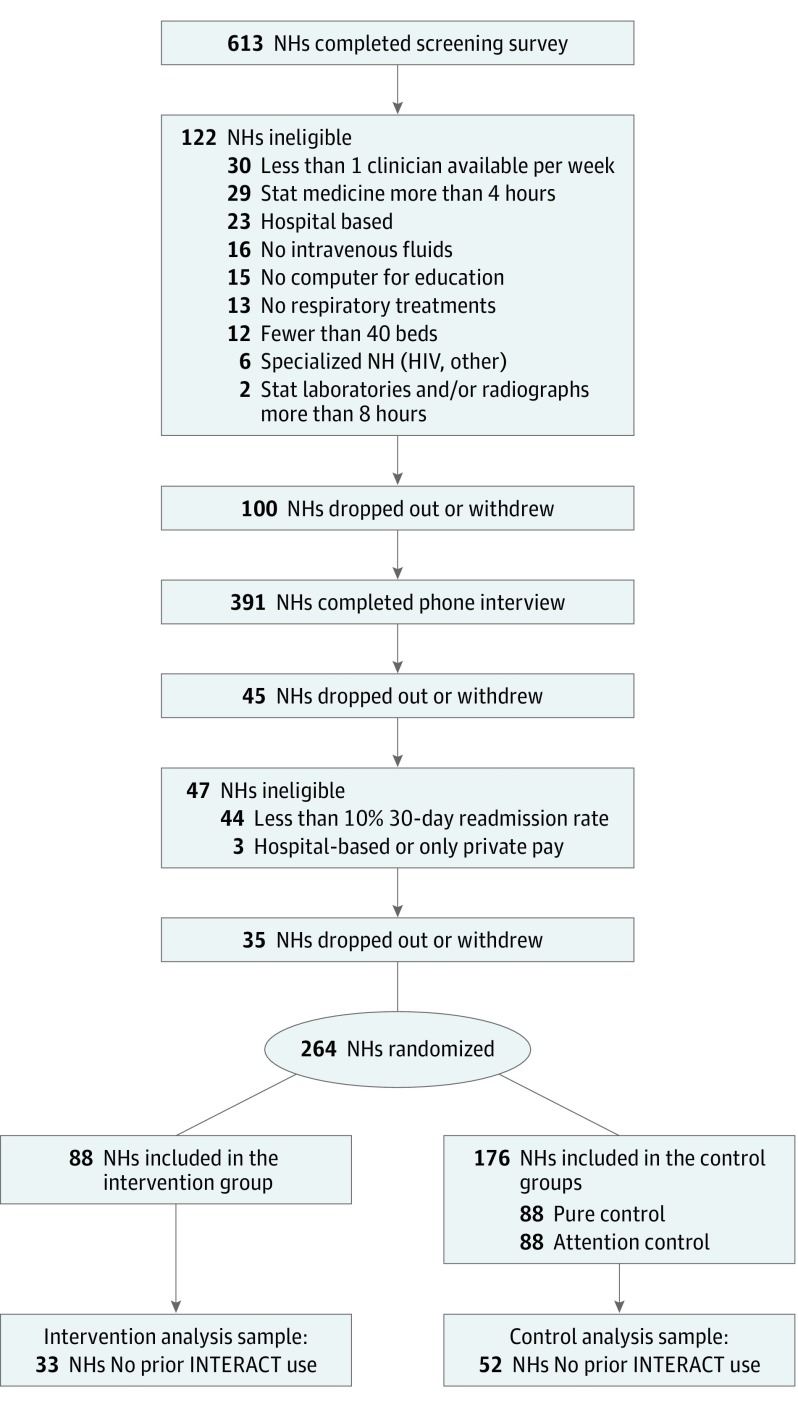
Design, setting, and participants: This analysis compared changes in hospitalization and ED visit rates between the preintervention and postintervention periods for NHs randomly assigned to receive training and implementation support on INTERACT to changes in control NHs. The analysis focused on 85 NHs (36 717 NH residents) that reported no use of INTERACT during the preintervention period.
Interventions: The study team provided training and support for implementing INTERACT, which included tools that help NH staff identify and evaluate acute changes in NH resident condition and document communication between physicians; care paths to avoid hospitalization when safe and feasible; and advance care planning and quality improvement tools.
Main outcomes and measures: All-cause hospitalizations, hospitalizations considered potentially avoidable, 30-day hospital readmissions, and ED visits without admission. All-cause hospitalization rates were calculated for all resident-days, high-risk days (0-30 days after NH admission), and lower-risk days (≥31 days after NH admission).
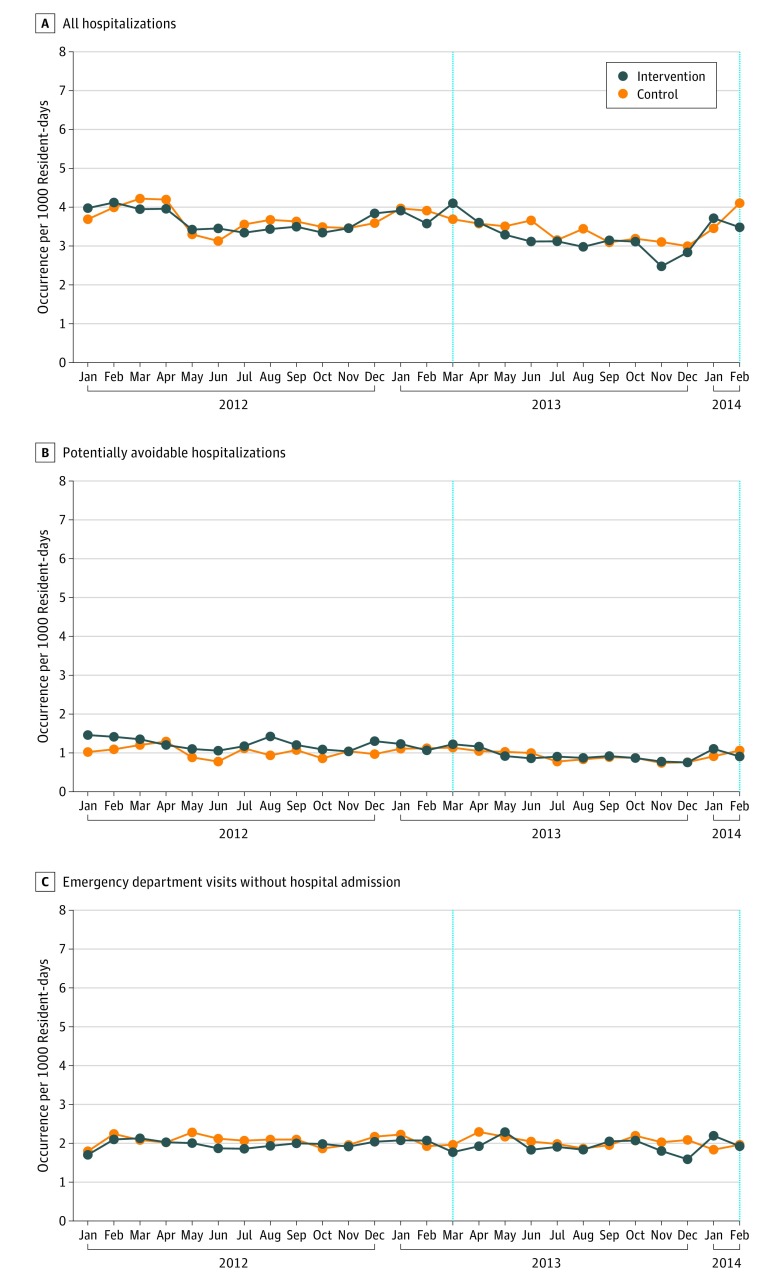
Results: We found that of 85 NHs, those that received implementation training and support exhibited statistically nonsignificant reductions in hospitalization rates compared with control NHs (net difference, -0.13 per 1000 resident-days; P = .25), hospitalizations during the first 30 days after NH admission (net difference, -0.37 per 1000 resident-days; P = .48), hospitalizations during periods more than 30 days after NH admission (net difference, -0.09 per 1000 resident-days; P = .39), 30-day readmission rates (net change in rate among hospital discharges, -0.01; P = .36), and ED visits without admission (net difference, 0.02 per 1000 resident-days; P = .83). Intervention NHs exhibited a reduction in potentially avoidable hospitalizations overall (net difference, -0.18 per 1000 resident-days, P = .01); however, this effect was not robust to a Bonferroni correction for multiple comparisons.
Conclusions and relevance: Training and support for INTERACT implementation as carried out in this study had no effect on hospitalization or ED visit rates in the overall population of residents in participating NHs. The results have several important implications for implementing quality improvement initiatives in NHs.
Trial registration: clinicaltrials.gov Identifier: NCT02177058.
Conflict of interest statement
Figures
References
-
- Department of Health and Human Services - Office of Inspector General Medicare Nursing Home Resident Hospitalization Rates Merit Additional Monitoring. https://oig.hhs.gov/oei/reports/oei-06-11-00040.asp Published November 18, 2013. Accessed May 17, 2017.
-
- Ackerly DC, Grabowski DC. Post-acute care reform—beyond the ACA. N Engl J Med. 2014;370(8):689-691. - PubMed
-
- Ouslander JG, Berenson RA. Reducing unnecessary hospitalizations of nursing home residents. N Engl J Med. 2011;365(13):1165-1167. - PubMed
-
- Ouslander JG, Lamb G, Perloe M, et al. Potentially avoidable hospitalizations of nursing home residents: frequency, causes, and costs [see editorial comments by Wyman JF and Hazzard WR, pp 760-761]. J Am Geriatr Soc. 2010;58(4):627-635. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
