

Effect of Insulin Degludec vs Insulin Glargine U100 on Hypoglycemia in Patients With Type 2 Diabetes: The SWITCH 2 Randomized Clinical Trial
- PMID: 28672317
- PMCID: PMC5817473
- DOI: 10.1001/jama.2017.7117
Effect of Insulin Degludec vs Insulin Glargine U100 on Hypoglycemia in Patients With Type 2 Diabetes: The SWITCH 2 Randomized Clinical Trial
Abstract
Importance: Hypoglycemia, a serious risk for insulin-treated patients with type 2 diabetes, negatively affects glycemic control.
Objective: To test whether treatment with basal insulin degludec is associated with a lower rate of hypoglycemia compared with insulin glargine U100 in patients with type 2 diabetes.
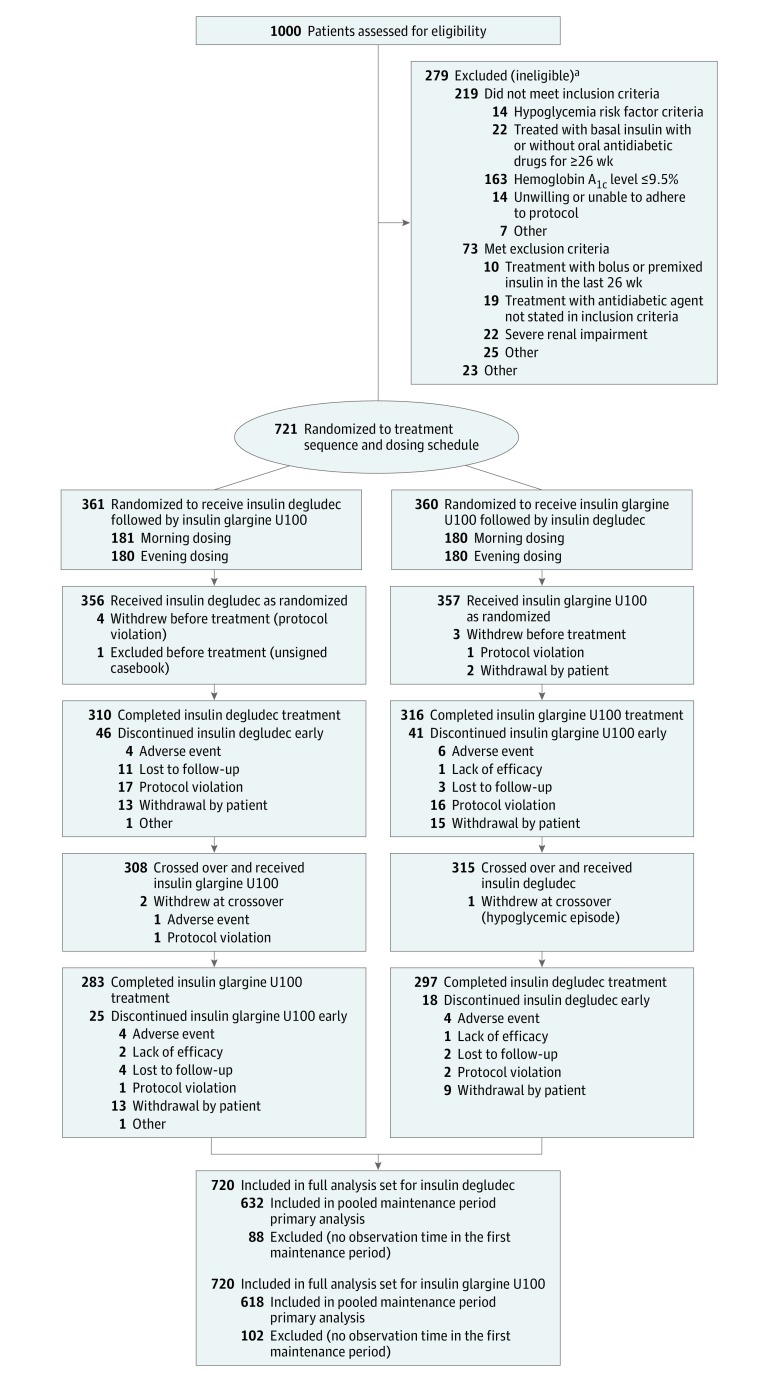
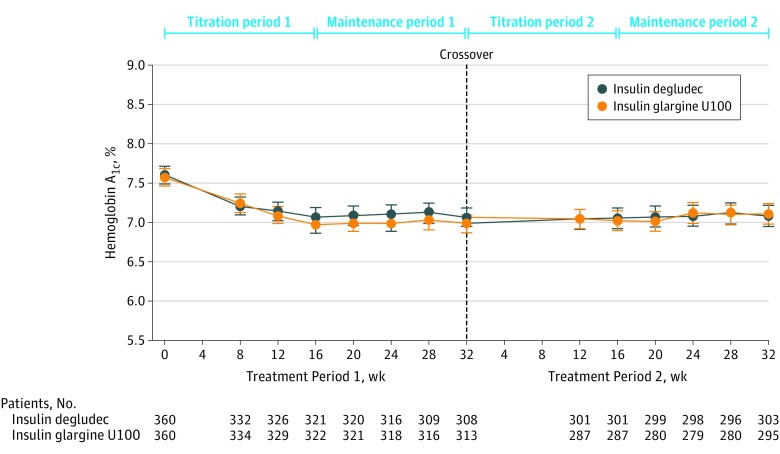
Design, setting, and participants: Randomized, double-blind, treat-to-target crossover trial including two 32-week treatment periods, each with a 16-week titration period and a 16-week maintenance period. The trial was conducted at 152 US centers between January 2014 and December 2015 in 721 adults with type 2 diabetes and at least 1 hypoglycemia risk factor who were previously treated with basal insulin with or without oral antidiabetic drugs.
Interventions: Patients were randomized 1:1 to receive once-daily insulin degludec followed by insulin glargine U100 (n = 361) or to receive insulin glargine U100 followed by insulin degludec (n = 360) and randomized 1:1 to morning or evening dosing within each treatment sequence.
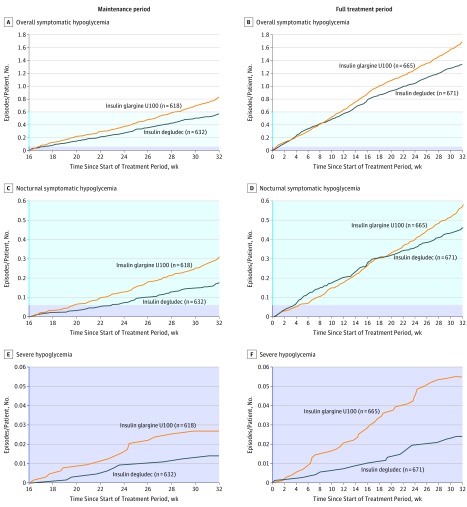
Main outcomes and measures: The primary end point was the rate of overall symptomatic hypoglycemic episodes (severe or blood glucose confirmed [<56 mg/dL]) during the maintenance period. Secondary end points were the rate of nocturnal symptomatic hypoglycemic episodes (severe or blood glucose confirmed, occurring between 12:01 am and 5:59 am) and the proportion of patients with severe hypoglycemia during the maintenance period.
Results: Of the 721 patients randomized (mean [SD] age, 61.4 [10.5] years; 53.1% male), 580 (80.4%) completed the trial. During the maintenance period, the rates of overall symptomatic hypoglycemia for insulin degludec vs insulin glargine U100 were 185.6 vs 265.4 episodes per 100 patient-years of exposure (PYE) (rate ratio = 0.70 [95% CI, 0.61-0.80]; P < .001; difference, -23.66 episodes/100 PYE [95% CI, -33.98 to -13.33]), and the proportions of patients with hypoglycemic episodes were 22.5% vs 31.6% (difference, -9.1% [95% CI, -13.1% to -5.0%]). The rates of nocturnal symptomatic hypoglycemia with insulin degludec vs insulin glargine U100 were 55.2 vs 93.6 episodes/100 PYE (rate ratio = 0.58 [95% CI, 0.46-0.74]; P < .001; difference, -7.41 episodes/100 PYE [95% CI, -11.98 to -2.85]), and the proportions of patients with hypoglycemic episodes were 9.7% vs 14.7% (difference, -5.1% [95% CI, -8.1% to -2.0%]). The proportions of patients experiencing severe hypoglycemia during the maintenance period were 1.6% (95% CI, 0.6%-2.7%) for insulin degludec vs 2.4% (95% CI, 1.1%-3.7%) for insulin glargine U100 (McNemar P = .35; risk difference, -0.8% [95% CI, -2.2% to 0.5%]). Statistically significant reductions in overall and nocturnal symptomatic hypoglycemia for insulin degludec vs insulin glargine U100 were also seen for the full treatment period.
Conclusions and relevance: Among patients with type 2 diabetes treated with insulin and with at least 1 hypoglycemia risk factor, 32 weeks' treatment with insulin degludec vs insulin glargine U100 resulted in a reduced rate of overall symptomatic hypoglycemia.
Trial registration: clinicaltrials.gov Identifier: NCT02030600.
Conflict of interest statement
Figures
Comment in
-
Hypoglycemia in Diabetes: Does Insulin Type Matter?JAMA. 2017 Jul 4;318(1):31-32. doi: 10.1001/jama.2017.8075. JAMA. 2017. PMID: 28672298 No abstract available.
Similar articles
-
Lower rates of hypoglycaemia in older individuals with type 2 diabetes using insulin degludec versus insulin glargine U100: Results from SWITCH 2.Diabetes Obes Metab. 2019 Jul;21(7):1634-1641. doi: 10.1111/dom.13708. Epub 2019 Apr 15. Diabetes Obes Metab. 2019. PMID: 30891886 Free PMC article. Clinical Trial.
-
Effect of Insulin Degludec vs Insulin Glargine U100 on Hypoglycemia in Patients With Type 1 Diabetes: The SWITCH 1 Randomized Clinical Trial.JAMA. 2017 Jul 4;318(1):33-44. doi: 10.1001/jama.2017.7115. JAMA. 2017. PMID: 28672316 Free PMC article. Clinical Trial.
-
Effect of insulin degludec versus insulin glargine U100 on time in range: SWITCH PRO, a crossover study of basal insulin-treated adults with type 2 diabetes and risk factors for hypoglycaemia.Diabetes Obes Metab. 2021 Nov;23(11):2572-2581. doi: 10.1111/dom.14504. Epub 2021 Aug 16. Diabetes Obes Metab. 2021. PMID: 34322967 Free PMC article. Clinical Trial.
-
(Ultra-)long-acting insulin analogues versus NPH insulin (human isophane insulin) for adults with type 2 diabetes mellitus.Cochrane Database Syst Rev. 2020 Nov 9;11(11):CD005613. doi: 10.1002/14651858.CD005613.pub4. Cochrane Database Syst Rev. 2020. PMID: 33166419 Free PMC article.
-
Comparative safety and efficacy of insulin degludec with insulin glargine in type 2 and type 1 diabetes: a meta-analysis of randomized controlled trials.Acta Diabetol. 2018 May;55(5):429-441. doi: 10.1007/s00592-018-1107-1. Epub 2018 Feb 8. Acta Diabetol. 2018. PMID: 29423761 Review.
Cited by
-
Heart failure with insulin degludec versus glargine U100 in patients with type 2 diabetes at high risk of cardiovascular disease: DEVOTE 14.Cardiovasc Diabetol. 2019 Nov 15;18(1):156. doi: 10.1186/s12933-019-0960-8. Cardiovasc Diabetol. 2019. PMID: 31729990 Free PMC article. Clinical Trial.
-
Personalized Management of Type 2 Diabetes.Curr Diab Rep. 2019 Nov 4;19(11):115. doi: 10.1007/s11892-019-1244-0. Curr Diab Rep. 2019. PMID: 31686226 Review.
-
Lower rates of hypoglycaemia in older individuals with type 2 diabetes using insulin degludec versus insulin glargine U100: Results from SWITCH 2.Diabetes Obes Metab. 2019 Jul;21(7):1634-1641. doi: 10.1111/dom.13708. Epub 2019 Apr 15. Diabetes Obes Metab. 2019. PMID: 30891886 Free PMC article. Clinical Trial.
-
Clinical outcomes in real-world patients with type 2 diabetes switching from first- to second-generation basal insulin analogues: Comparative effectiveness of insulin glargine 300 units/mL and insulin degludec in the DELIVER D+ cohort study.Diabetes Obes Metab. 2018 Sep;20(9):2148-2158. doi: 10.1111/dom.13345. Epub 2018 Jun 25. Diabetes Obes Metab. 2018. PMID: 29938887 Free PMC article.
-
Appropriate Titration of Basal Insulin in Type 2 Diabetes and the Potential Role of the Pharmacist.Adv Ther. 2019 May;36(5):1031-1051. doi: 10.1007/s12325-019-00907-8. Epub 2019 Mar 21. Adv Ther. 2019. PMID: 30900198 Free PMC article. Review.
References
-
- Frier BM. How hypoglycaemia can affect the life of a person with diabetes. Diabetes Metab Res Rev. 2008;24(2):87-92. - PubMed
-
- Leiter LA, Yale JF, Chiasson JL, Harris S, Kleinstiver P, Sauriol L. Assessment of the impact of fear of hypoglycemic episodes on glycemic and hypoglycemia management. Can J Diabetes. 2005;29(3):186-192.
-
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577-1589. - PubMed
-
- Nathan DM, Buse JB, Davidson MB, et al. ; American Diabetes Association; European Association for Study of Diabetes . Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32(1):193-203. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
