

Cardiovascular disease risk profiles in inflammatory joint disease entities
- PMID: 28673314
- PMCID: PMC5496163
- DOI: 10.1186/s13075-017-1358-1
Cardiovascular disease risk profiles in inflammatory joint disease entities
Abstract
Background: Patients with inflammatory joint diseases (IJD) have increased risk of cardiovascular disease (CVD). Our aim was to compare CVD risk profiles in patients with IJD, including rheumatoid arthritis (RA), axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) and evaluate the future risk of CVD.
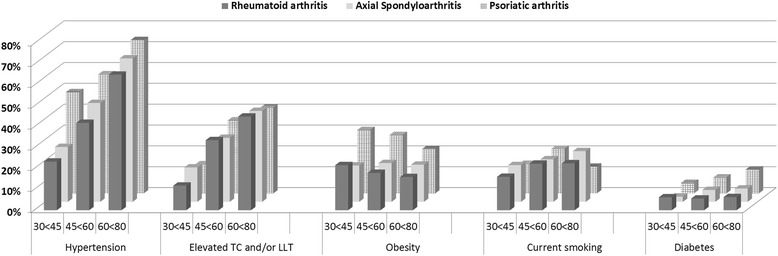
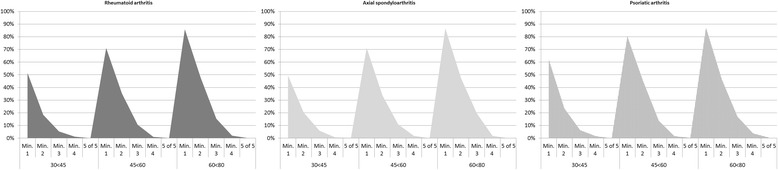
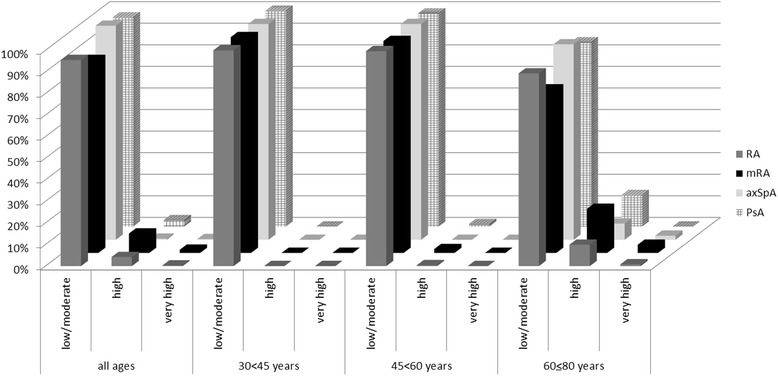
Methods: The prevalence and numbers of major CVD risk factors (CVD-RFs) (hypertension, elevated cholesterol, obesity, smoking, and diabetes mellitus) were estimated in patients with RA, axSpA and PsA. Relative and absolute risk of CVD according to Systematic Coronary Risk Evaluation (SCORE) was calculated.
Results: In total, 3791 patients were included. CVD was present in 274 patients (7.2%). Of those without established CVD; hypertension and elevated cholesterol were the most frequent CVD-RFs, occurring in 49.8% and 32.8% of patients. Patients with PsA were more often hypertensive and obese. Overall, 73.6% of patients had a minimum of one CVD-RF, which increased from 53.2% among patients aged 30 to <45 years, to 86.2% of patients aged 60 to ≤80 years. Most patients (93.5%) had low/moderate estimated risk of CVD according to SCORE. According to relative risk estimations, 35.2% and 24.7% of patients had two or three times risk or higher, respectively, compared to individuals with no CVD-RFs.
Conclusions: In this nationwide Norwegian project, we have shown for the first time that prevalence and numbers of CVD-RFs were relatively comparable across the three major IJD entities. Furthermore, estimated absolute CVD risk was low, but the relative risk of CVD was markedly high in patients with IJD. Our findings indicate the need for CVD risk assessment in all patients with IJD.
Keywords: Cardiovascular; Epidemiology; Rheumatoid arthritis; Spondyloarthritis; Spondyloarthropathies.
Figures

Similar articles
-
Discrepancies in risk age and relative risk estimations of cardiovascular disease in patients with inflammatory joint diseases.Int J Cardiol. 2018 Feb 1;252:201-206. doi: 10.1016/j.ijcard.2017.10.038. Int J Cardiol. 2018. PMID: 29249429
-
Cardiovascular morbidity and associated risk factors in Spanish patients with chronic inflammatory rheumatic diseases attending rheumatology clinics: Baseline data of the CARMA Project.Semin Arthritis Rheum. 2015 Jun;44(6):618-26. doi: 10.1016/j.semarthrit.2014.12.002. Epub 2014 Dec 25. Semin Arthritis Rheum. 2015. PMID: 26058345
-
Guideline recommended treatment to targets of cardiovascular risk is inadequate in patients with inflammatory joint diseases.Int J Cardiol. 2019 Jan 1;274:311-318. doi: 10.1016/j.ijcard.2018.06.111. Epub 2018 Jul 2. Int J Cardiol. 2019. PMID: 30007486
-
Sex and Cardiovascular Involvement in Inflammatory Joint Diseases.Clin Rev Allergy Immunol. 2019 Jun;56(3):278-292. doi: 10.1007/s12016-017-8635-2. Clin Rev Allergy Immunol. 2019. PMID: 28852999 Review.
-
EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update.Ann Rheum Dis. 2017 Jan;76(1):17-28. doi: 10.1136/annrheumdis-2016-209775. Epub 2016 Oct 3. Ann Rheum Dis. 2017. PMID: 27697765 Review.
Cited by
-
Evolving Management of Low-Density Lipoprotein Cholesterol: A Personalized Approach to Preventing Atherosclerotic Cardiovascular Disease Across the Risk Continuum.J Am Heart Assoc. 2023 Jun 6;12(11):e028892. doi: 10.1161/JAHA.122.028892. Epub 2023 Jun 1. J Am Heart Assoc. 2023. PMID: 37260036 Free PMC article. Review.
-
Myocardial infarction & C-reactive protein levels among Mexican adults with arthritis: Findings from the Mexican Health and Aging Study.Int J Cardiol Cardiovasc Risk Prev. 2024 Jul 3;22:200309. doi: 10.1016/j.ijcrp.2024.200309. eCollection 2024 Sep. Int J Cardiol Cardiovasc Risk Prev. 2024. PMID: 39055965 Free PMC article.
-
Prediction of cardiovascular events in rheumatoid arthritis using risk age calculations: evaluation of concordance across risk age models.Arthritis Res Ther. 2020 Apr 23;22(1):90. doi: 10.1186/s13075-020-02178-z. Arthritis Res Ther. 2020. PMID: 32326974 Free PMC article.
-
Cardiovascular Risks and Risk Stratification in Inflammatory Joint Diseases: A Cross-Sectional Study.Front Med (Lausanne). 2022 Feb 22;9:786776. doi: 10.3389/fmed.2022.786776. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35280915 Free PMC article.
-
Perioperative medical management for patients with RA, SPA, and SLE undergoing total hip and total knee replacement: a narrative review.BMC Rheumatol. 2018 Jan 30;2:2. doi: 10.1186/s41927-018-0008-9. eCollection 2018. BMC Rheumatol. 2018. PMID: 30886953 Free PMC article. Review.
References
-
- Horreau C, Pouplard C, Brenaut E, Barnetche T, Misery L, Cribier B, Jullien D, Aractingi S, Aubin F, Joly P, et al. Cardiovascular morbidity and mortality in psoriasis and psoriatic arthritis: a systematic literature review. J Eur Acad Dermatol Venereol. 2013;27(Suppl 3):12–29. doi: 10.1111/jdv.12163. - DOI - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney MT, Corra U, Cosyns B, Deaton C, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) Eur Heart J. 2016;252:207–74. - PubMed
-
- Agca R, Heslinga SC, Rollefstad S, Heslinga M, McInnes IB, Peters MJ, Kvien TK, Dougados M, Radner H, Atzeni F, et al. EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann Rheum Dis. 2017;76.1:17–28. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
