

Open-chest versus closed-chest cardiopulmonary resuscitation in blunt trauma: analysis of a nationwide trauma registry
- PMID: 28673321
- PMCID: PMC5496413
- DOI: 10.1186/s13054-017-1759-1
Open-chest versus closed-chest cardiopulmonary resuscitation in blunt trauma: analysis of a nationwide trauma registry
Abstract
Background: Although open-chest cardiopulmonary resuscitation (OCCPR) is often considered as the last salvage maneuver in critically injured patients, evidence on the effectiveness of OCCPR has been based only on the descriptive studies of limited numbers of cases or expert opinions. This study aimed to compare the effectiveness of OCCPR with that of closed-chest cardiopulmonary resuscitation (CCCPR) in an emergency department (ED).
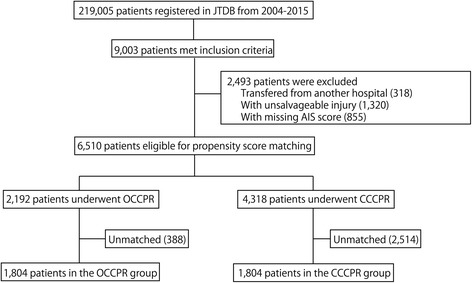
Methods: A nationwide registry-based, retrospective cohort study was conducted. Patients with blunt trauma, undergoing cardiopulmonary resuscitation (CPR) in an ED between 2004 and 2015 were identified and divided into OCCPR and CCCPR groups. Their outcomes (survival to hospital discharge and survival over 24 hours following ED arrival) were compared with propensity score matching analysis and instrumental variable analysis.
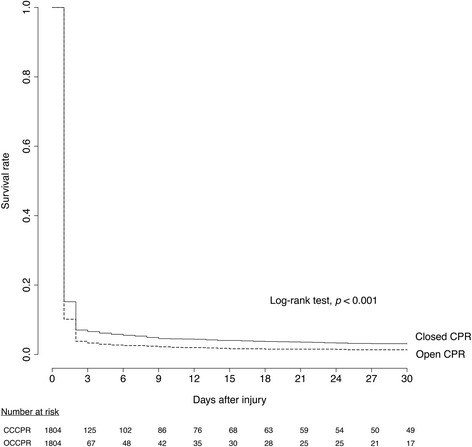
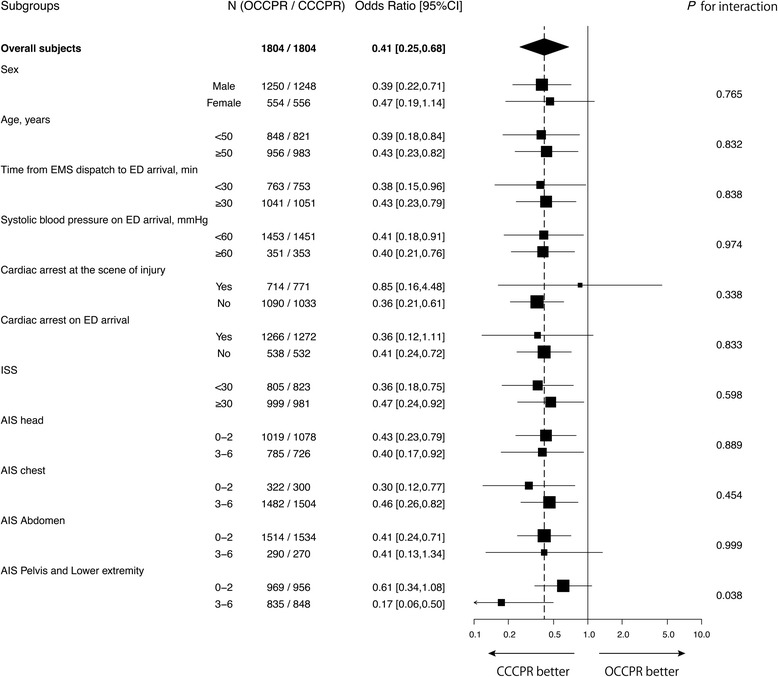
Results: A total of 6510 patients (OCCPR, 2192; CCCPR, 4318) were analyzed. The in-hospital and 24-hour survival rates in OCCPR patients were 1.8% (40/2192) and 5.6% (123/2192), and those in CCCPR patients were 3.6% (156/4318) and 9.6% (416/4318), respectively. In the propensity score-matched subjects, OCCPR patients (n = 1804) had significantly lower odds of survival to hospital discharge (odds ratio (95% CI)) = 0.41 (0.25-0.68)) and of survival over 24 hours following ED arrival (OR (95% CI) = 0.59 (0.45-0.79)) than CCCPR patients (n = 1804). Subgroup analysis revealed that OCCPR was associated with a poorer outcome compared to CCCPR in patients with severe pelvis and lower extremity injury.
Conclusions: In this large cohort, OCCPR was associated with reduced in-hospital and 24-hour survival rates in patients with blunt trauma. Further comparisons between OCCPR and CCCPR using additional information, such as time course details in pre-hospital and ED settings, anatomical details regarding region of injury, and neurological outcomes, are necessary.
Keywords: Cardiac arrest; Emergency thoracotomy; Polytrauma; Registry; Resuscitation; Shock.
Conflict of interest statement
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Limited evidence to recommend against open chest cardiopulmonary resuscitation in blunt trauma.Crit Care. 2017 Sep 20;21(1):244. doi: 10.1186/s13054-017-1831-x. Crit Care. 2017. PMID: 28931419 Free PMC article. No abstract available.
References
-
- Mazzorana V, Smith RS, Morabito DJ, Brar HS. Limited utility of emergency department thoracotomy. Am Surg. 1994;60:520–1. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
