

Is Cardioprotection Dead?
- PMID: 28674094
- PMCID: PMC5814253
- DOI: 10.1161/CIRCULATIONAHA.116.027039
Is Cardioprotection Dead?
Abstract
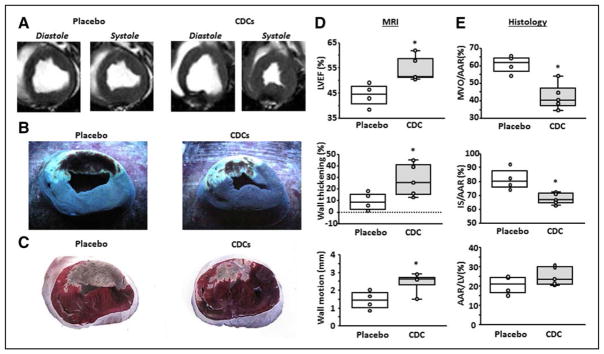
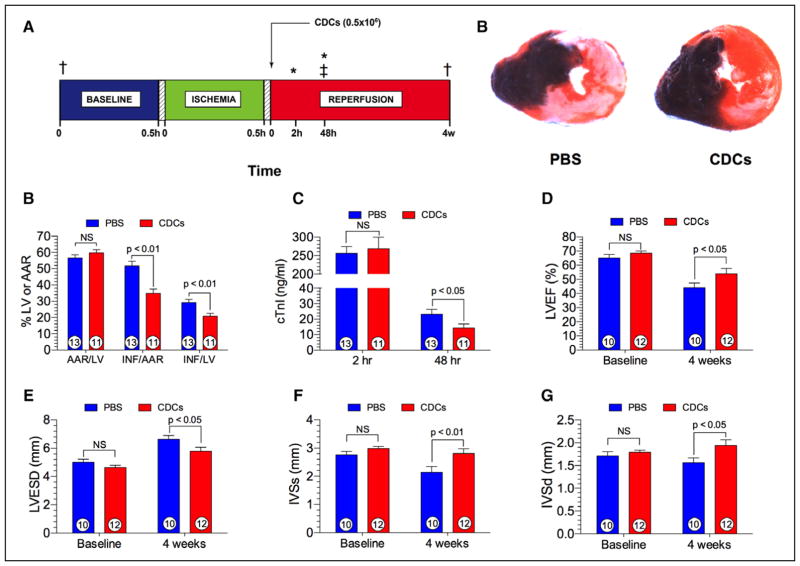
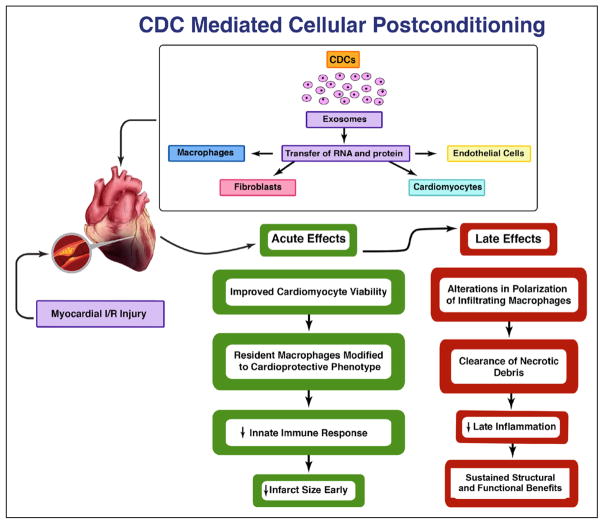
For >4 decades, the holy grail in the treatment of acute myocardial infarction has been the mitigation of lethal injury. Despite promising initial results and decades of investigation by the cardiology research community, the only treatment with proven efficacy is early reperfusion of the occluded coronary artery. The remarkable record of failure has led us and others to wonder if cardioprotection is dead. The path to translation, like the ascent to Everest, is certainly littered with corpses. We do, however, highlight a therapeutic principle that provides a glimmer of hope: cellular postconditioning. Administration of cardiosphere-derived cells after reperfusion limits infarct size measured acutely, while providing long-term structural and functional benefits. The recognition that cell therapy may be cardioprotective, and not just regenerative, merits further exploration before we abandon the pursuit entirely.
Keywords: cardiosphere derived cells; cell- and tissue-based therapy; heart failure; myocardial Infarction; ventricular function, left.
© 2017 American Heart Association, Inc.
Figures
References
-
- Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation. 1990;81:1161–1172. - PubMed
-
- St John Sutton M, Pfeffer MA, Plappert T, Rouleau JL, Moyé LA, Dagenais GR, Lamas GA, Klein M, Sussex B, Goldman S. Quantitative two-dimensional echocardiographic measurements are major predictors of adverse cardiovascular events after acute myocardial infarction. The protective effects of captopril. Circulation. 1994;89:68–75. - PubMed
-
- Reimer KA, Jennings RB. Failure of the xanthine oxidase inhibitor allopurinol to limit infarct size after ischemia and reperfusion in dogs. Circulation. 1985;71:1069–1075. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
