

Aspects on the Physiological and Biochemical Foundations of Neurocritical Care
- PMID: 28674514
- PMCID: PMC5474476
- DOI: 10.3389/fneur.2017.00274
Aspects on the Physiological and Biochemical Foundations of Neurocritical Care
Abstract
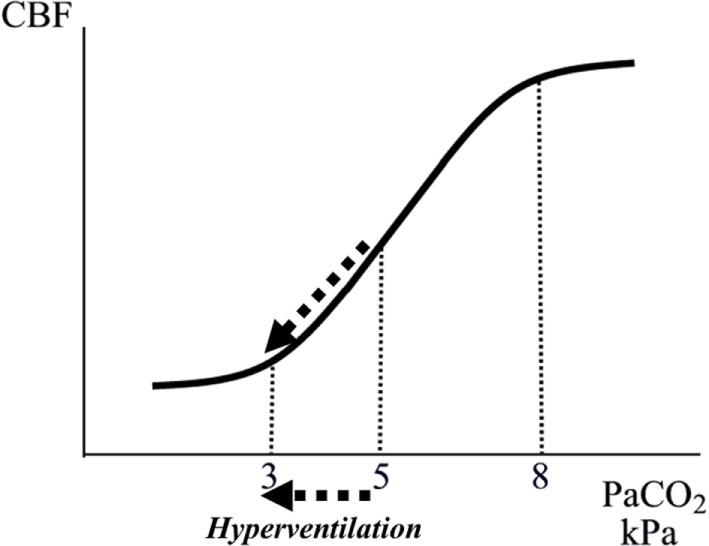
Neurocritical care (NCC) is a branch of intensive care medicine characterized by specific physiological and biochemical monitoring techniques necessary for identifying cerebral adverse events and for evaluating specific therapies. Information is primarily obtained from physiological variables related to intracranial pressure (ICP) and cerebral blood flow (CBF) and from physiological and biochemical variables related to cerebral energy metabolism. Non-surgical therapies developed for treating increased ICP are based on knowledge regarding transport of water across the intact and injured blood-brain barrier (BBB) and the regulation of CBF. Brain volume is strictly controlled as the BBB permeability to crystalloids is very low restricting net transport of water across the capillary wall. Cerebral pressure autoregulation prevents changes in intracranial blood volume and intracapillary hydrostatic pressure at variations in arterial blood pressure. Information regarding cerebral oxidative metabolism is obtained from measurements of brain tissue oxygen tension (PbtO2) and biochemical data obtained from intracerebral microdialysis. As interstitial lactate/pyruvate (LP) ratio instantaneously reflects shifts in intracellular cytoplasmatic redox state, it is an important indicator of compromised cerebral oxidative metabolism. The combined information obtained from PbtO2, LP ratio, and the pattern of biochemical variables reveals whether impaired oxidative metabolism is due to insufficient perfusion (ischemia) or mitochondrial dysfunction. Intracerebral microdialysis and PbtO2 give information from a very small volume of tissue. Accordingly, clinical interpretation of the data must be based on information of the probe location in relation to focal brain damage. Attempts to evaluate global cerebral energy state from microdialysis of intraventricular fluid and from the LP ratio of the draining venous blood have recently been presented. To be of clinical relevance, the information from all monitoring techniques should be presented bedside online. Accordingly, in the future, the chemical variables obtained from microdialysis will probably be analyzed by biochemical sensors.
Keywords: cerebral blood flow; cerebral energy metabolism; intracranial pressure; microdialysis; neurocritical care.
Figures











References
-
- Lundberg N. Continuous recording and control of ventricular pressure in neurosurgical practice. Acta Psychiatr Scand Suppl (1960) 36:1–93. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials