

The systolic paradox in hypertrophic cardiomyopathy
- PMID: 28674623
- PMCID: PMC5471858
- DOI: 10.1136/openhrt-2016-000571
The systolic paradox in hypertrophic cardiomyopathy
Abstract
Objective: We explored cardiac volumes and the effects on systolic function in hypertrophic cardiomyopathy (HCM) patients with left ventricular hypertrophy (HCM LVH+) and genotype-positive patients without left ventricular hypertrophy (HCM LVH-).
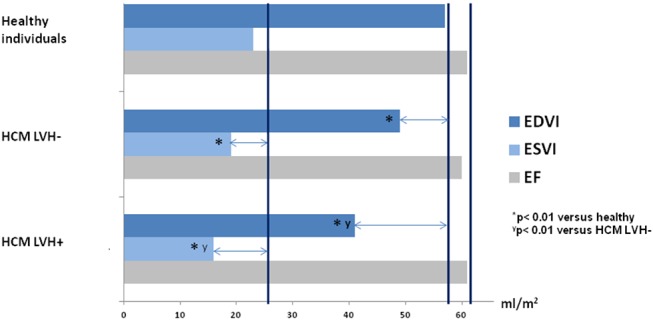
Methods: We included 180 HCM LVH+, 100 HCM LVH- patients and 80 healthy individuals. End-Diastolic Volume Index (EDVI), End-Systolic Volume Index (ESVI) and ejection fraction (EF) were assessed by echocardiography. Left ventricular (LV) global longitudinal strain (GLS) was measured by speckle tracking echocardiography.
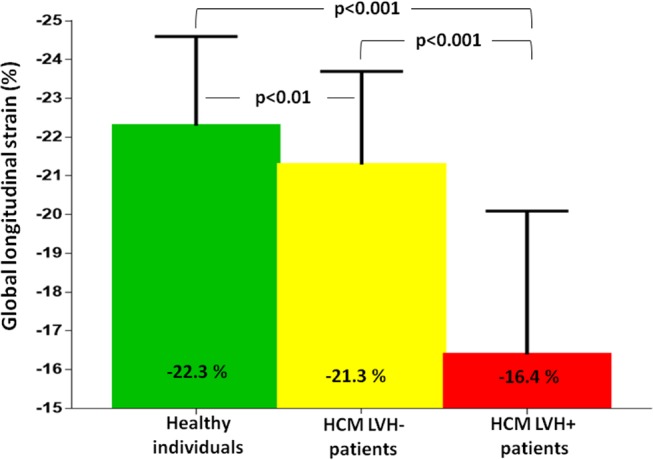
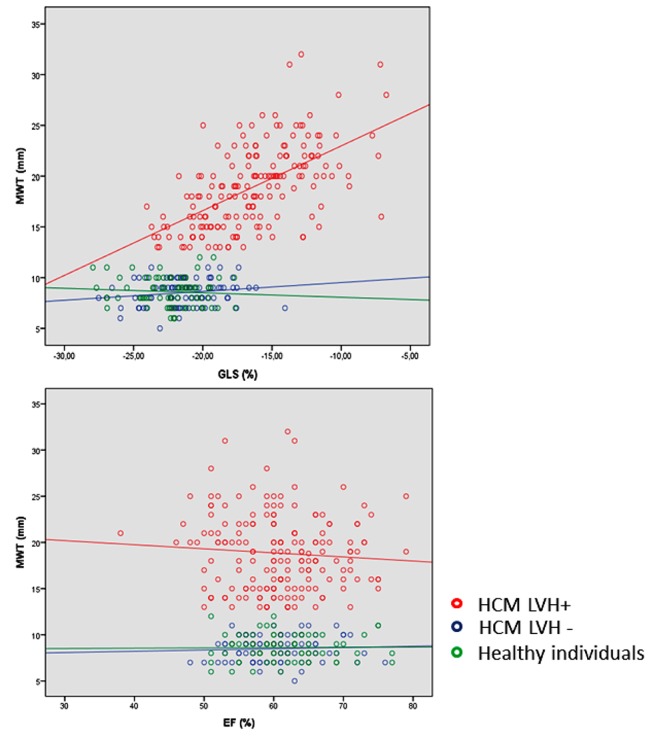
Results: EDVI and ESVI were significantly smaller in HCM LVH+ compared with HCM LVH- patients (41±14 mL/m2 vs 49±13 mL/m2 and 16±7 mL/m2 vs 19±6 mL/m2, respectively, both p<0.001) and in healthy individuals (41±14 mL/m2 vs 57±14 mL/m2 and 16±7 mL/m2 vs 23±9 mL/m2, respectively, both p<0.001). HCM LVH- patients had significantly lower EDVI and ESVI compared with healthy individuals (49±13 mL/m2 vs 57±14 mL/m2 and 19±6 mL/m2 vs 23±9 mL/m2, both p<0.001). EF was similar (61%±7% vs 60%±8% vs 61%±6%, p=0.43) in the HCM LVH+, HCM LVH- and healthy individuals, despite significantly worse GLS in the HCM LVH+ (-16.4%±3.7% vs -21.3%±2.4% vs -22.3%±3.7%, p<0.001). GLS was worse in the HCM LVH- compared with healthy individuals in pairwise comparison (p=0.001). Decrease in ESVI was closely related to EF in HCM LVH+ and HCM LVH- (R=0.45, p<0.001 and R=0.43, p<0.001) as expected, but there was no relationship with GLS (R=0.02, p=0.77 and R=0.11, p=0.31). Increased maximal wall thickness (MWT) correlated significantly with worse GLS (R=0.58, p<0.001), but not with EF (R=0.018, p=0.30) in the HCM LVH+ patients.
Conclusion: HCM LVH+ had smaller cardiac volumes that could explain the preserved EF, despite worse GLS that was closely related to MWT. HCM LVH- had reduced cardiac volumes and subtle changes in GLS compared with healthy individuals, indicating a continuum of both volumetric and systolic changes present before increased MWT.
Keywords: Hypertrophic cardiomyopathy; echocardiography and heart failure with preserved ejection fraction.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Echocardiographic characteristics of PRKAG2 syndrome: a research using three-dimensional speckle tracking echocardiography compared with sarcomeric hypertrophic cardiomyopathy.Cardiovasc Ultrasound. 2022 May 5;20(1):14. doi: 10.1186/s12947-022-00284-3. Cardiovasc Ultrasound. 2022. PMID: 35509080 Free PMC article.
-
Strain analysis during exercise in patients with left ventricular hypertrophy: impact of etiology.J Am Soc Echocardiogr. 2013 Oct;26(10):1163-1169. doi: 10.1016/j.echo.2013.06.002. Epub 2013 Jul 13. J Am Soc Echocardiogr. 2013. PMID: 23860095
-
Left ventricular dyssynchrony and 2D and 3D global longitudinal strain for differentiating physiological and pathological left ventricular hypertrophy.Arch Cardiovasc Dis. 2017 Jun-Jul;110(6-7):403-412. doi: 10.1016/j.acvd.2016.11.003. Epub 2017 Jan 3. Arch Cardiovasc Dis. 2017. PMID: 28065448
-
Prognostic Value of Global Longitudinal Strain in Hypertrophic Cardiomyopathy: A Systematic Review of Existing Literature.JACC Cardiovasc Imaging. 2019 Oct;12(10):1930-1942. doi: 10.1016/j.jcmg.2018.07.016. Epub 2018 Sep 12. JACC Cardiovasc Imaging. 2019. PMID: 30219395
-
Differentiating the athlete's heart from hypertrophic cardiomyopathy.Curr Opin Cardiol. 2015 Sep;30(5):500-5. doi: 10.1097/HCO.0000000000000203. Curr Opin Cardiol. 2015. PMID: 26196658 Review.
Cited by
-
A multi-scale finite element method for investigating fiber remodeling in hypertrophic cardiomyopathy.Sci Rep. 2025 Aug 30;15(1):31961. doi: 10.1038/s41598-025-17778-5. Sci Rep. 2025. PMID: 40885813 Free PMC article.
-
Fabry Disease: More than a Phenocopy of Hypertrophic Cardiomyopathy.J Clin Med. 2023 Nov 13;12(22):7061. doi: 10.3390/jcm12227061. J Clin Med. 2023. PMID: 38002674 Free PMC article. Review.
-
Aortic annular plane systolic excursion in cats with hypertrophic cardiomyopathy.J Vet Intern Med. 2024 Jan-Feb;38(1):61-70. doi: 10.1111/jvim.16962. Epub 2023 Dec 1. J Vet Intern Med. 2024. PMID: 38038190 Free PMC article.
-
An In Silico Cardiomyocyte Reveals the Impact of Changes in CaMKII Signalling on Cardiomyocyte Contraction Kinetics in Hypertrophic Cardiomyopathy.Biomed Res Int. 2024 Mar 25;2024:6160554. doi: 10.1155/2024/6160554. eCollection 2024. Biomed Res Int. 2024. PMID: 38567164 Free PMC article.
-
Right ventricular function declines prior to left ventricular ejection fraction in hypertrophic cardiomyopathy.J Cardiovasc Magn Reson. 2022 Jun 13;24(1):36. doi: 10.1186/s12968-022-00868-y. J Cardiovasc Magn Reson. 2022. PMID: 35692049 Free PMC article.
References
-
- Elliott PM, Anastasakis A, Borger MA, et al. . Authors/Task Force members. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J 2014;35:2733–79.10.1093/eurheartj/ehu284 - DOI - PubMed
-
- Cardim N, Galderisi M, Edvardsen T, et al. . Role of multimodality cardiac imaging in the management of patients with hypertrophic cardiomyopathy: an expert consensus of the European Association of Cardiovascular Imaging endorsed by the Saudi Heart Association. Eur Heart J Cardiovasc Imaging 2015;16:280laboratories, and age matched with HCM LVH+ patients.All participants gave written informed consent. Thestudy complied with the Declaration of Helsinki andwas approved by the Regional Committees for MedicalResearch Ethicslaboratories, and age matched with HCM LVH+ patients.All participants gave written informed consent. Thestudy complied with the Declaration of Helsinki andwas approved by the Regional Committees for MedicalResearch Ethics10.1093/ehjci/jeu291 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous