

Morbidity outcomes after surgical aortic valve replacement
- PMID: 28674629
- PMCID: PMC5471875
- DOI: 10.1136/openhrt-2017-000588
Morbidity outcomes after surgical aortic valve replacement
Abstract
Objective: In patients with mild to moderate operative risk, surgical aortic valve replacement (SAVR) is still the preferred treatment for patients with severe symptomatic aortic stenosis (AS). Aiming to broaden the knowledge of postsurgical outcomes, this study reports a broad set of morbidity outcomes following surgical intervention.
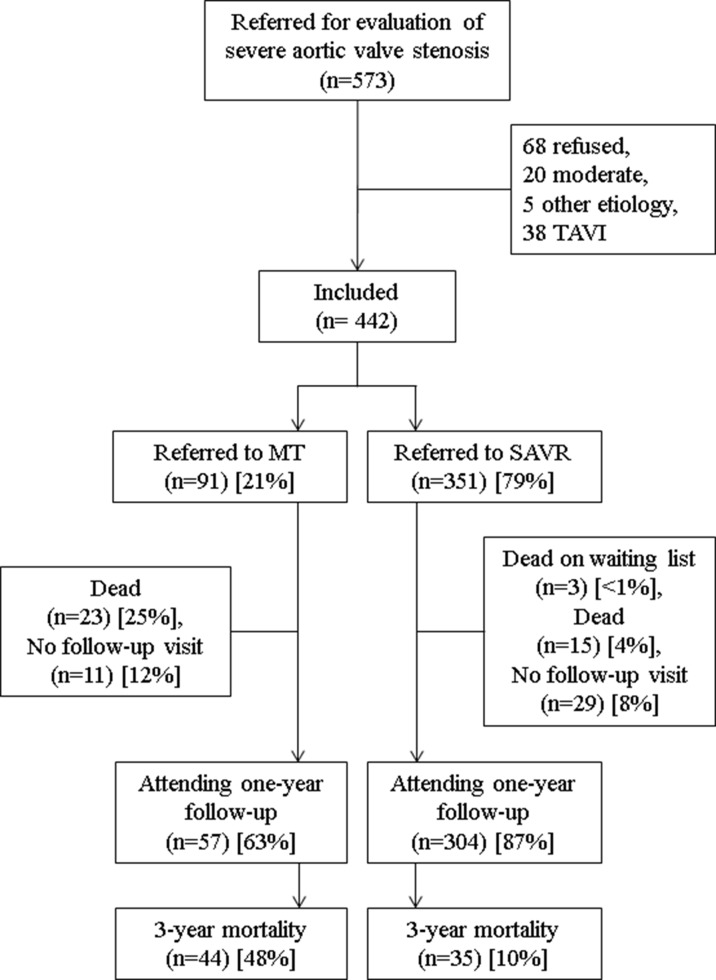
Methods: Our cohort comprised 442 patients referred for severe AS; 351 had undergone SAVR, with the remainder (91) not operated on. All patients were evaluated using the 6-minute walk test (6MWT), were assigned a New York Heart Association class (NYHA) and Canadian Cardiovascular Society class (CCS), with additional scores for health-related quality of life (HRQoL), cognitive function (Mini-Mental State Examination (MMSE)) and myocardial remodelling (at inclusion and at 1-year follow-up). Adverse events and mortality were recorded.
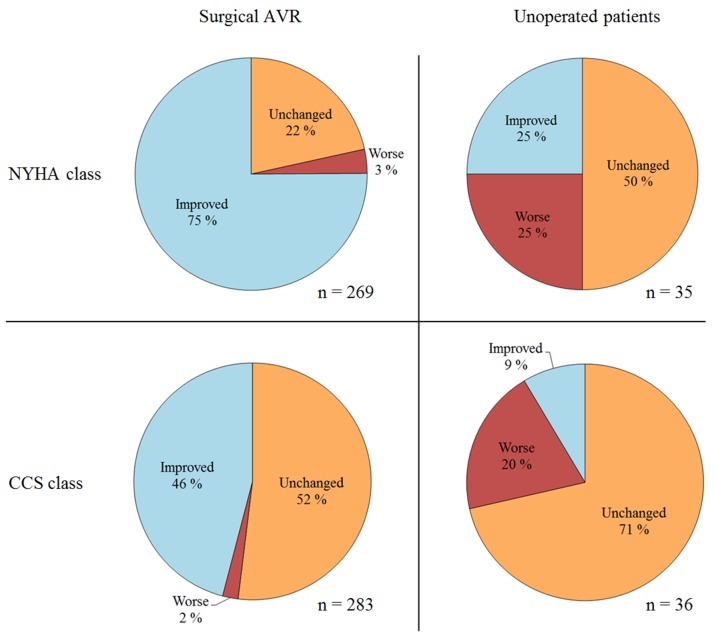
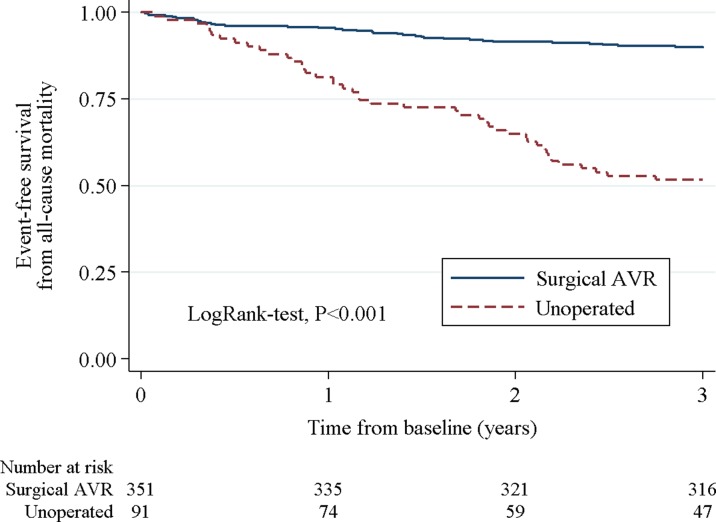
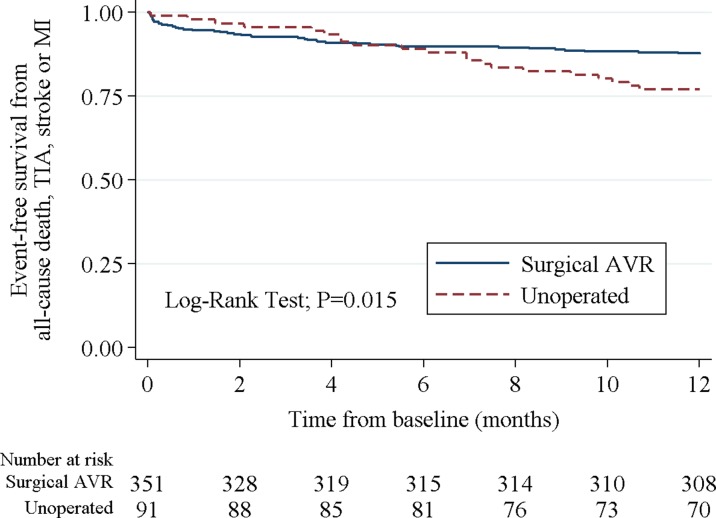
Results: Three-year survival after SAVR was 90.0%. SAVR was associated with an improved NYHA class, CCS score and HRQoL, and provoked reverse ventricular remodelling. The 6MWT decreased, while the risks of major adverse cardiovascular events (death, non-fatal stroke/transient ischaemic attack or myocardial infarction) and all-cause hospitalisation (incidence rate per 100 patient-years) were 13.5 and 62.4, respectively. The proportion of cognitive disability measured by MMSE increased after SAVR from 3.2% to 8.8% (p=0.005). Proportion of patients living independently at home, having attained NYHA class I, was met by 49.1% at 1 year. Unoperated individuals had a poor prognosis in terms of any outcome.
Conclusion: This study provides knowledge of outcomes beyond what is known about the mortality benefit after SAVR to provide insight into the morbidity burden of modern-day SAVR.
Keywords: Aortic valvne disease; Quality of care and outcomes; Surgery -valve.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Nishimura RA, Otto CM, Bonow RO, et al. AHA/ACC guideline for the management of patients with valvular heart disease.J Thorac Cardiovasc Surg 2014;2014:e1–e132. - PubMed
-
- Vahanian A, Alfieri O, Andreotti F, et al. ; Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) European Association for Cardio-Thoracic Surgery (EACTS). Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012;33:2451–96. 10.1093/eurheartj/ehs109 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous