

The Role of Central Neck Lymph Node Dissection in the Management of Papillary Thyroid Cancer
- PMID: 28674675
- PMCID: PMC5474838
- DOI: 10.3389/fonc.2017.00122
The Role of Central Neck Lymph Node Dissection in the Management of Papillary Thyroid Cancer
Abstract
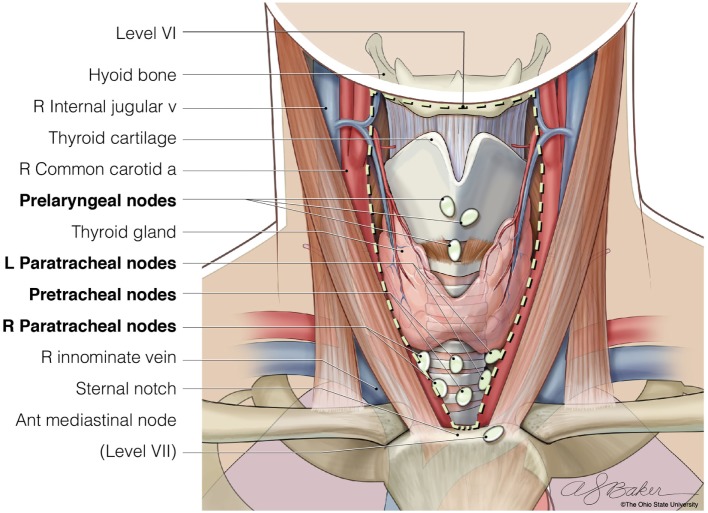
Papillary thyroid cancer (PTC) is the most common thyroid malignancy, and cervical nodal metastases are frequent at presentation. The most common site for nodal metastases from PTC is the central compartment of the ipsilateral neck in the paratracheal and pretracheal regions. The decision to resect these lymph nodes at the time of thyroidectomy often depends on if nodes with suspected malignancy can be identified preoperatively. If nodal spread to the central neck nodes is known, then the consensus is to remove all nodes in this area. However, there remains significant controversy regarding the utility of removing central neck lymph nodes for prophylactic reasons. Herein, we review the potential utility of central neck lymph node dissection as well as the risks of performing this procedure. As well, we review the potential of molecular testing to stratify patients who would most benefit from this procedure. We advocate a selective approach in which patients undergo clinical neck examination coupled with ultrasound to detect any concerning lymph nodes that warrant additional evaluation with either fine needle aspiration or excisional biopsy in the operating room. In lieu of clinical lymphadenopathy, we suggest the use of patient and disease characteristics as identified by multiple groups, such as the American Thyroid Association and European Society of Endocrine Surgeons, which include extremes of ages, large primary tumor size, and male gender, when deciding to perform central neck lymph node dissection. Patients should be educated on the potential long-terms risks versus the lack of known long-term benefits.
Keywords: central neck dissection; lymph nodes; papillary thyroid cancer; prophylactic surgery; surgical complications.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials