

Superior GVHD-free, relapse-free survival for G-BM to G-PBSC grafts is associated with higher MDSCs content in allografting for patients with acute leukemia
- PMID: 28676100
- PMCID: PMC5496166
- DOI: 10.1186/s13045-017-0503-2
Superior GVHD-free, relapse-free survival for G-BM to G-PBSC grafts is associated with higher MDSCs content in allografting for patients with acute leukemia
Abstract
Background: Granulocyte colony-stimulating factor (G-CSF)-mobilized peripheral blood stem cells (G-PBSC) has largely replaced unstimulated bone marrow (un-BM) for allografting because of accelerated engraftment, but with a higher morbidity and mortality of graft-versus-host-disease (GVHD). Recent studies suggested that G-CSF-primed BM (G-BM) had similar engraftment but lower morbidity and mortality of GVHD comparing to G-PBSC. A prospective, randomized, multicenter study was conducted to compare G-BM with G-PBSC as the grafts in allogeneic hematopoietic stem cell transplantation (allo-HSCT) for acute leukemia in first complete remission (CR1).
Methods: Totally 101 adult leukemia in CR1 undergoing HLA-identical sibling transplants were randomized into G-BM or G-PBSC group. The primary study endpoint was GVHD-free/relapse-free survival (GRFS).
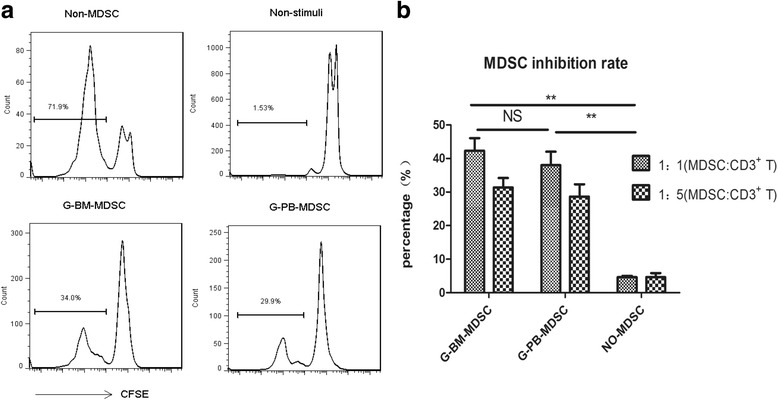
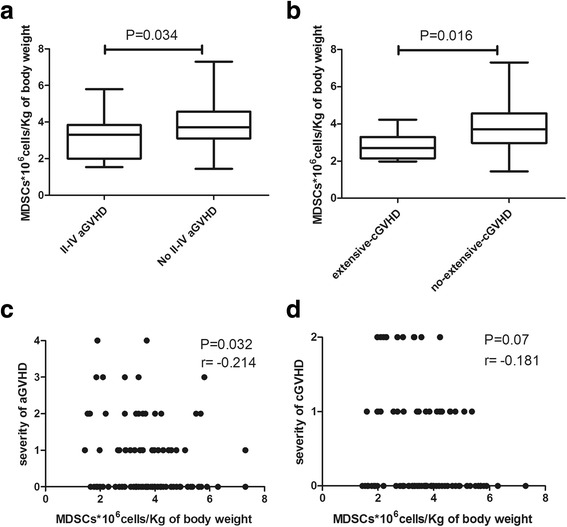
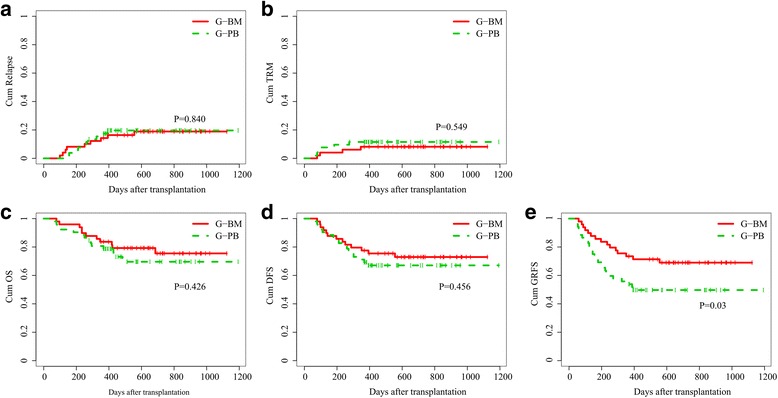
Results: Both the engraftment of neutrophil and platelet were 2 days later in G-BM than in G-PBSC group (P = 0.412, P = 0.39). G-BM group showed significantly lower II-IV acute GVHD (aGVHD) and similar III-IV aGVHD compared with G-PBSC group (12.2% vs 28.8% for II-IV, P = 0.048; 4.1% vs 9.6% for III-IV aGVHD, P = 0.267, respectively). The overall cumulative incidence of chronic GVHD (cGVHD) at 3 years were 22.3% ± 6.3% and 44.8% ± 7.6% (P = 0.026), respectively, and extensive cGHVD were 4.5% ± 3.1% and 15% ± 5.3% (P = 0.08), respectively, in G-BM and G-PBSC groups. Two groups had similar 3-year relapse, transplant-related mortality (TRM), overall survival (OS), and disease-free survival (DFS) (all P > 0.05). G-BM group showed significantly higher probability of GRFS than G-PBSC group (73.5% ± 6.3% vs 55.8% ± 6.9% at 1 year, P = 0.049; 69.0% ± 6.7% vs 49.7% ± 7.0% at 2 and 3 years, P = 0.03, respectively). Graft content analysis revealed statistically higher frequency of myeloid-derived suppressor cells (MDSCs) in the G-BM than in G-PBSC grafts (P < 0.01), and recipients received statistically higher numbers of MDSCs in G-BM than in G-PBSC group (P = 0.045). Numbers of MDSCs infused to patients were negatively correlated with the severity of aGVHD (P = 0.032, r = -0.214). Multivariate analysis showed that MDSC cell dose below the median (HR = 3.49, P < 0.001), recipient age (HR = 2.02, P = 0.039), and high risk of disease (HR = 2.14, P = 0.018) were independent risk factors for GRFS.
Conclusions: G-BM grafts lead a better GRFS and less GVHD associated with a higher MDSCs content compared with G-PBSC grafts.
Keywords: GVHD-free/relapse-free survival; Graft-versus-host disease; Granulocyte colony-stimulating factor (G-CSF)-primed bone marrow; Myeloid-derived suppressor cells.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the respective Ethics Committee of Nanfang Hospital, the First People’s Hospital of Chenzhou, People’s Hospital of Zhongshan City, and Concord Hospital of the Fujian Medical University. Written informed consent was obtained from all the subjects in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Schmitz N, Dreger P, Suttorp M, Rohwedder EB, Haferlach T, Loffler H, Hunter A, Russell NH. Primary transplantation of allogeneic peripheral blood progenitor cells mobilized by filgrastim (granulocyte colony-stimulating factor) Blood. 1995;85(6):1666–1672. - PubMed
-
- Majolino I, Saglio G, Scime R, Serra A, Cavallaro AM, Fiandaca T, Vasta S, Pampinella M, Catania P, Indovina A, et al. High incidence of chronic GVHD after primary allogeneic peripheral blood stem cell transplantation in patients with hematologic malignancies. Bone Marrow Transplant. 1996;17(4):555–560. - PubMed
-
- Pan L, Delmonte JJ, Jalonen CK, Ferrara J. Pretreatment of donor mice with granulocyte colony-stimulating factor polarizes donor T lymphocytes toward type-2 cytokine production and reduces severity of experimental graft-versus-host disease. Blood. 1995;86(12):4422–4429. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
